

Hepatocellular carcinoma with macrovascular invasion: multimodality imaging features for the diagnosis
- PMID: 32990243
- PMCID: PMC7664740
- DOI: 10.5152/dir.2020.19569
Hepatocellular carcinoma with macrovascular invasion: multimodality imaging features for the diagnosis
Abstract
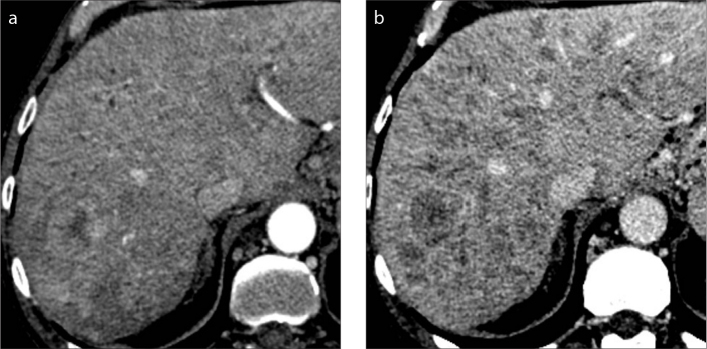
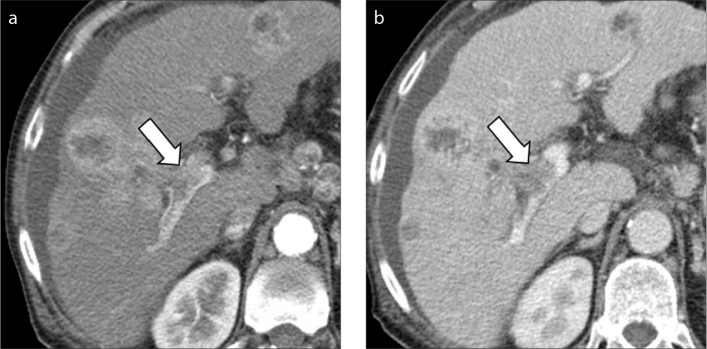
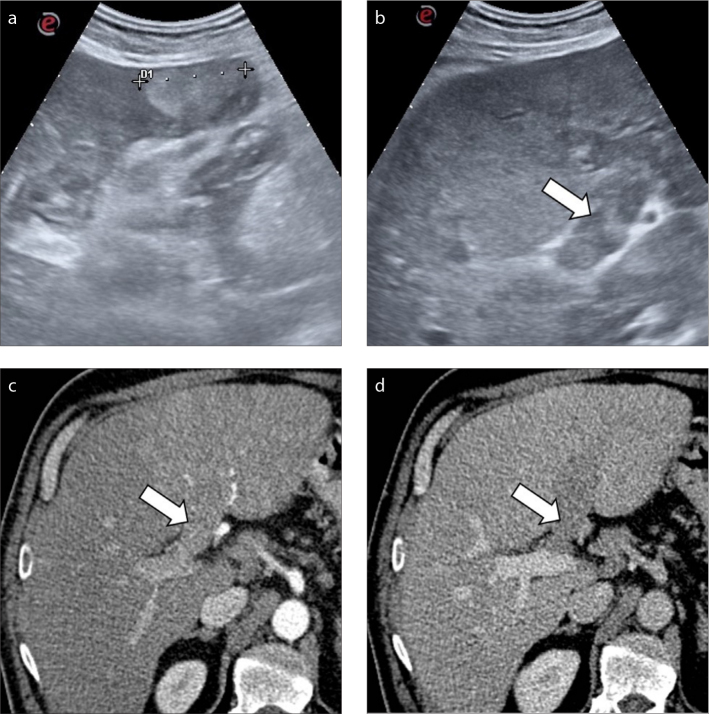
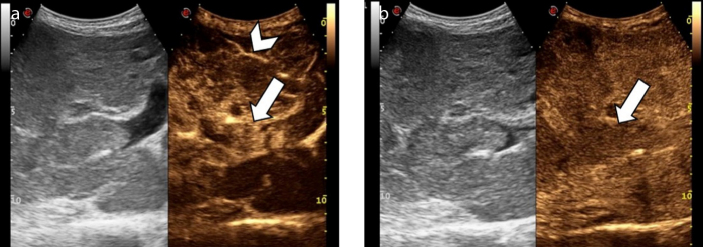
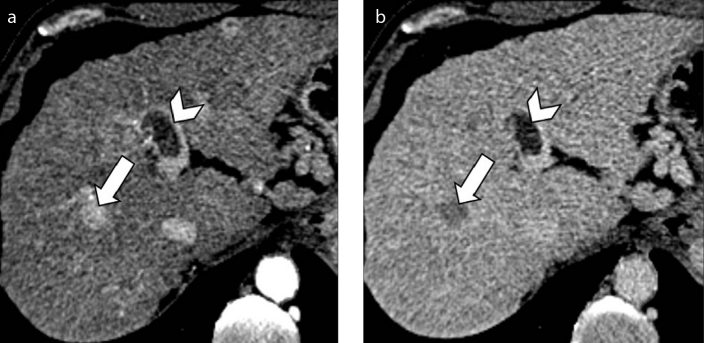
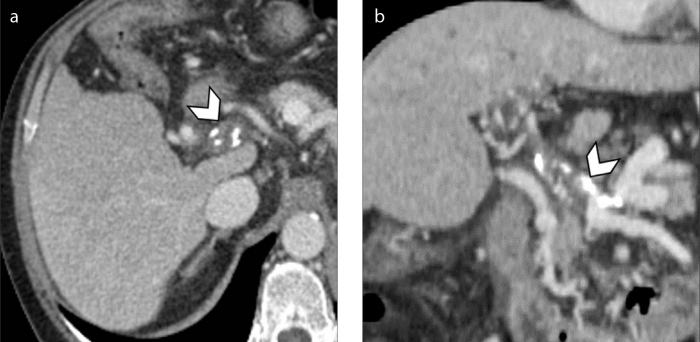
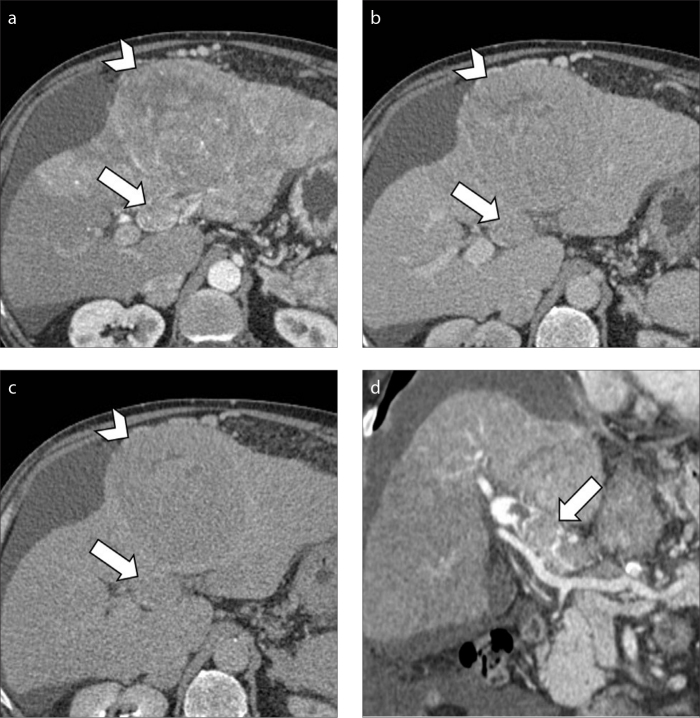
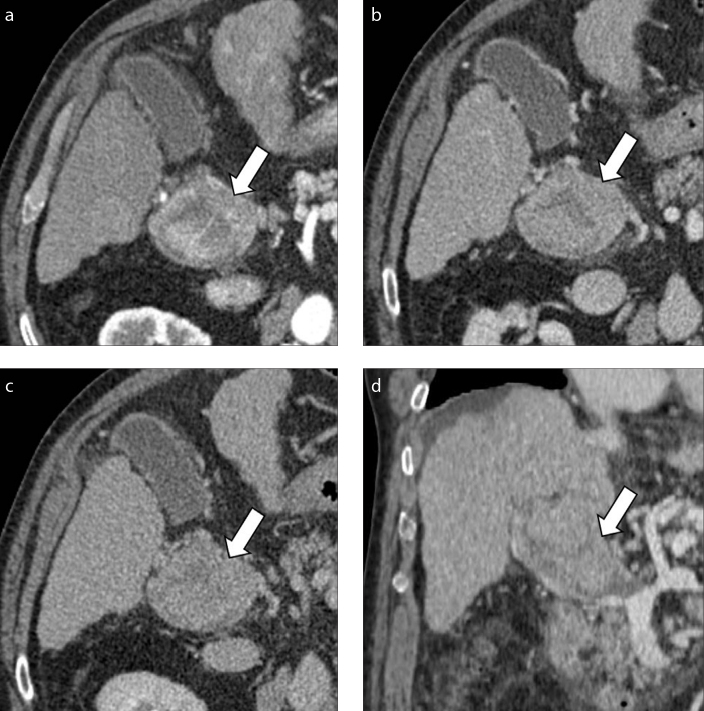
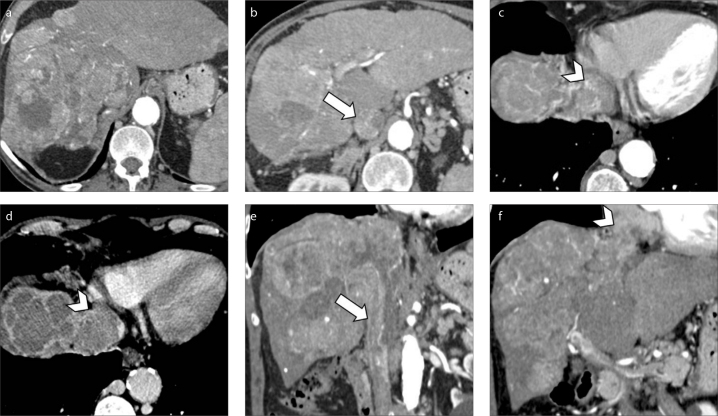
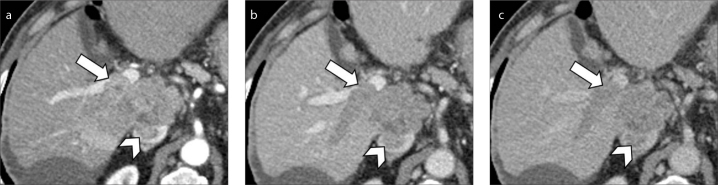
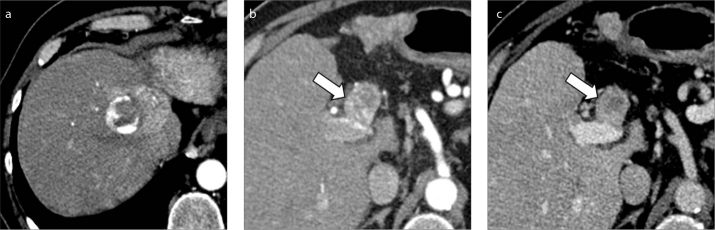
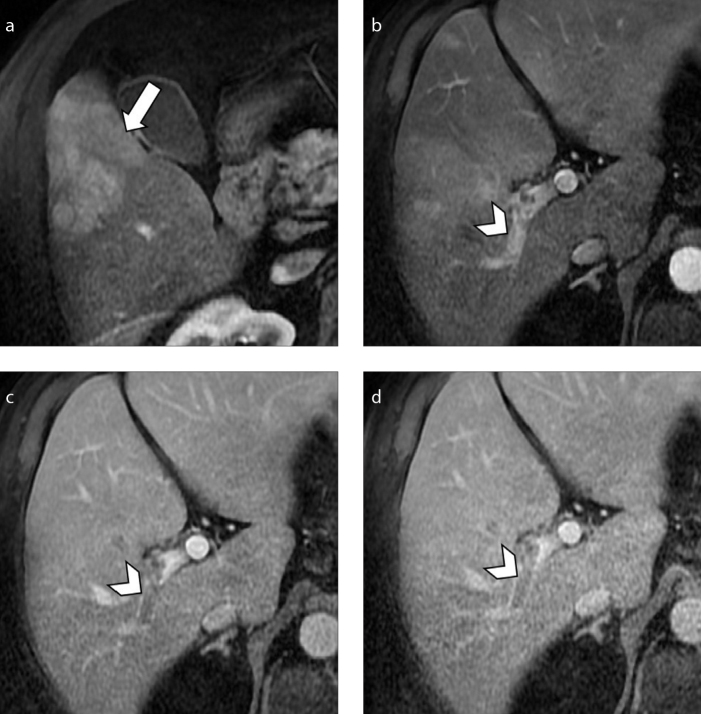
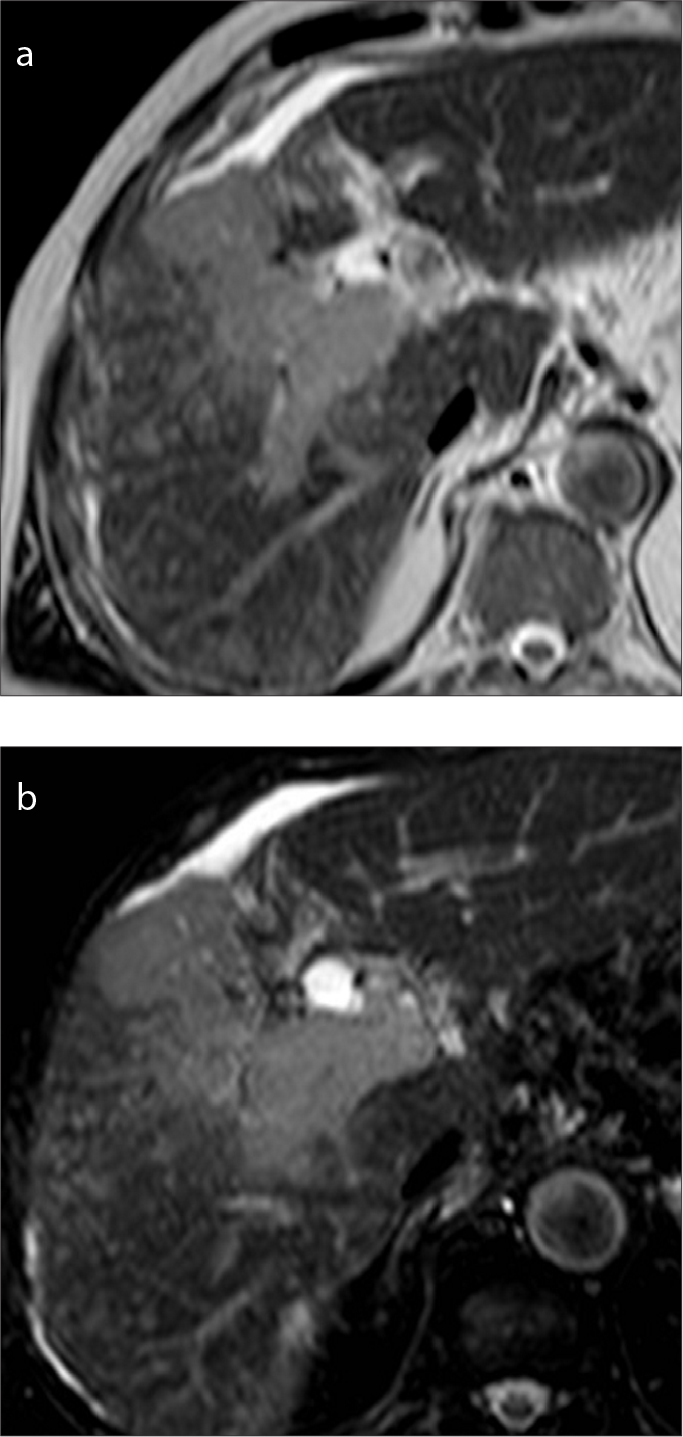
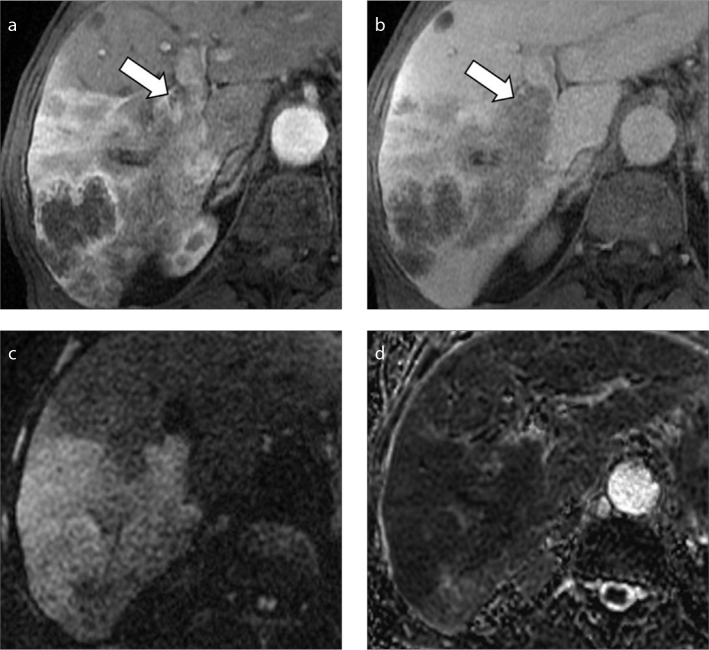
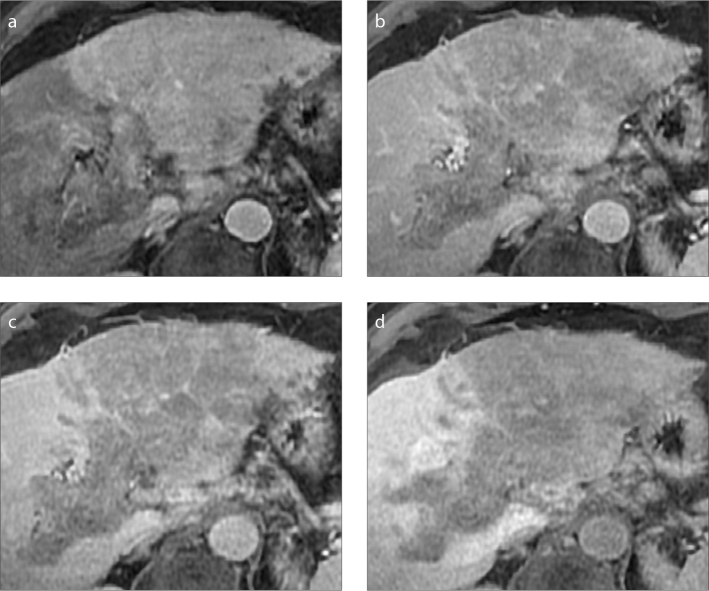
Hepatocellular carcinoma (HCC) is frequently associated with macrovascular invasion of the portal vein or hepatic veins in advanced stages. The accurate diagnosis of macrovascular invasion and the differentiation from bland non-tumoral thrombus has significant clinical and management implications, since it narrows the therapeutic options and it represents a mandatory contraindication for liver resection or transplantation. The imaging diagnosis remains particularly challenging since the imaging features of HCC with macrovascular invasion may be subtle, especially in lesions showing infiltrative appearance. However, each radiologic imaging modality may provide findings suggesting the presence of tumor thrombus rather than bland thrombus. The purpose of this paper is to review the current guidelines and imaging appearance of HCC with macrovascular invasion. Knowledge of the most common imaging features of HCC with macrovascular invasion may improve the diagnostic confidence of tumor thrombus in clinical practice and help to guide patients' management.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures

References
-
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
