

Recurrent YAP1 and MAML2 Gene Rearrangements in Retiform and Composite Hemangioendothelioma
- PMID: 32991341
- PMCID: PMC7773139
- DOI: 10.1097/PAS.0000000000001575
Recurrent YAP1 and MAML2 Gene Rearrangements in Retiform and Composite Hemangioendothelioma
Abstract
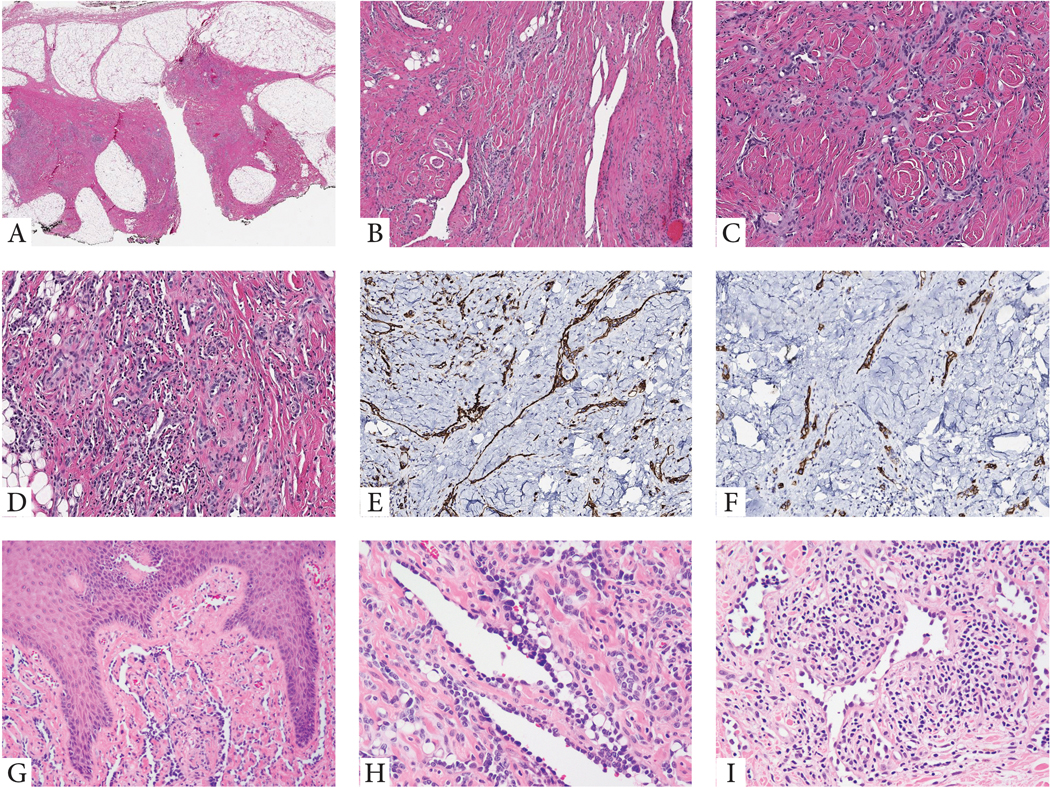
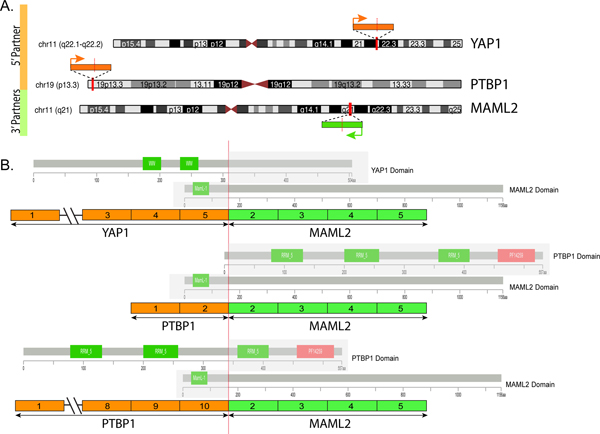
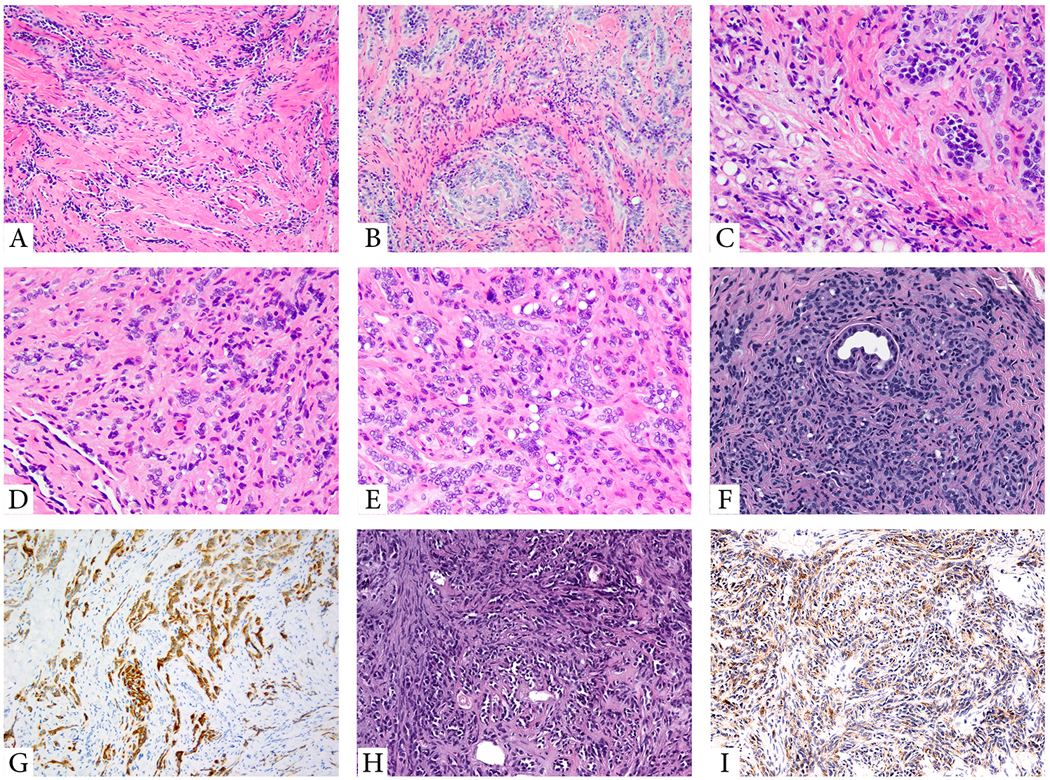
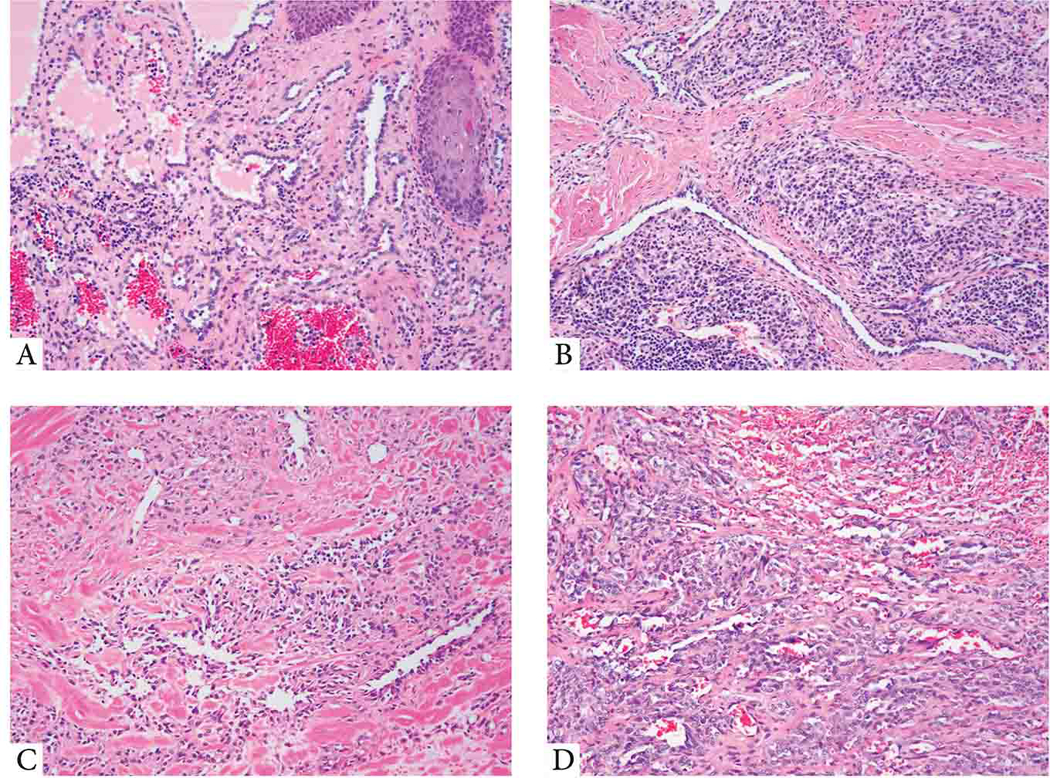
Retiform and composite hemangioendotheliomas (CHEs) are both locally aggressive, rarely metastasizing vascular neoplasms characterized by arborizing vascular channels lined by endothelial cells with a hobnail morphology. CHE displays additional cytologic and architectural components, including often vacuolated epithelioid cells, solid areas, or features reminiscent of well-differentiated angiosarcoma. Triggered by an index case of a soft tissue retiform hemangioendothelioma (RHE) which revealed a YAP1-MAML2 gene fusion by targeted RNA sequencing, we sought to investigate additional cases in this morphologic spectrum for this genetic abnormality. A total of 24 cases, 13 RHE and 11 CHE involving skin and soft tissue were tested by fluorescence in situ hybridization using custom BAC probes for rearrangements involving these genes. An additional visceral CHE with neuroendocrine differentiation was tested by targeted RNA sequencing. Among the soft tissue cohort, 5/13 (38%) RHE and 3/11 (27%) CHE showed YAP1 gene rearrangements, with 5 cases showing a YAP1-MAML2 fusion, including all 3 CHE. The single neuroendocrine CHE showed the presence of a PTBP1-MAML2 fusion. All YAP1-positive CHE lesions occurred in female children at acral sites, compared with fusion-negative cases which occurred in adults, with a wide anatomic distribution. YAP1-positive RHE occurred preferentially in males and lower limb, compared with negative cases. These results suggest that RHE and CHE represent a morphologic continuum, sharing abnormalities in YAP1 and MAML2 genes. In contrast, the neuroendocrine CHE occurring in a 37-year-old male harbored a distinct PTBP1-MAML2 fusion and showed aggressive clinical behavior (pancreatic mass with multiple liver and lung metastases). These preliminary findings raise the possibility that neuroendocrine CHE may be genetically distinct from the conventional RHE/CHE spectrum. Further studies are needed to investigate the pathogenetic relationship of fusion-negative cases with this subset and, less likely, with other members of the HE family of tumors.
Conflict of interest statement
Figures
References
-
- Rubin BP. Composite haemangioendothelioma In: Fletcher CD, Bridge JA, Pancras CW, et al. [eds]. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon, France: IARC Press; 2013.
-
- Nayler SJ, Rubin BP, Calonje E, et al. Composite hemangioendothelioma: a complex, low-grade vascular lesion mimicking angiosarcoma. Am J Surg Pathol. 2000;24:352–361. - PubMed
-
- Perry KD, Al-Lbraheemi A, Rubin BP, et al. Composite hemangioendothelioma with neuroendocrine marker expression: an aggressive variant. Mod Pathol. 2017;30:1589–1602. - PubMed
-
- Shang Leen SL, Fisher C, Thway K. Composite hemangioendothelioma: clinical and histologic features of an enigmatic entity. Adv Anat Pathol. 2015;22:254–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
