

Emerging Causes of Drug-Induced Anaphylaxis: A Review of Anaphylaxis-Associated Reports in the FDA Adverse Event Reporting System (FAERS)
- PMID: 32992044
- PMCID: PMC7870524
- DOI: 10.1016/j.jaip.2020.09.021
Emerging Causes of Drug-Induced Anaphylaxis: A Review of Anaphylaxis-Associated Reports in the FDA Adverse Event Reporting System (FAERS)
Abstract
Background: Drug-induced anaphylaxis is a well-known adverse drug reaction for some drug classes, but emerging drug causes of anaphylaxis and novel mechanisms may contribute in unrecognized ways.
Objective: We sought to determine the top drugs reported in association with anaphylaxis and anaphylaxis followed by death in the Food and Drug Administration Adverse Event Reporting System (FAERS).
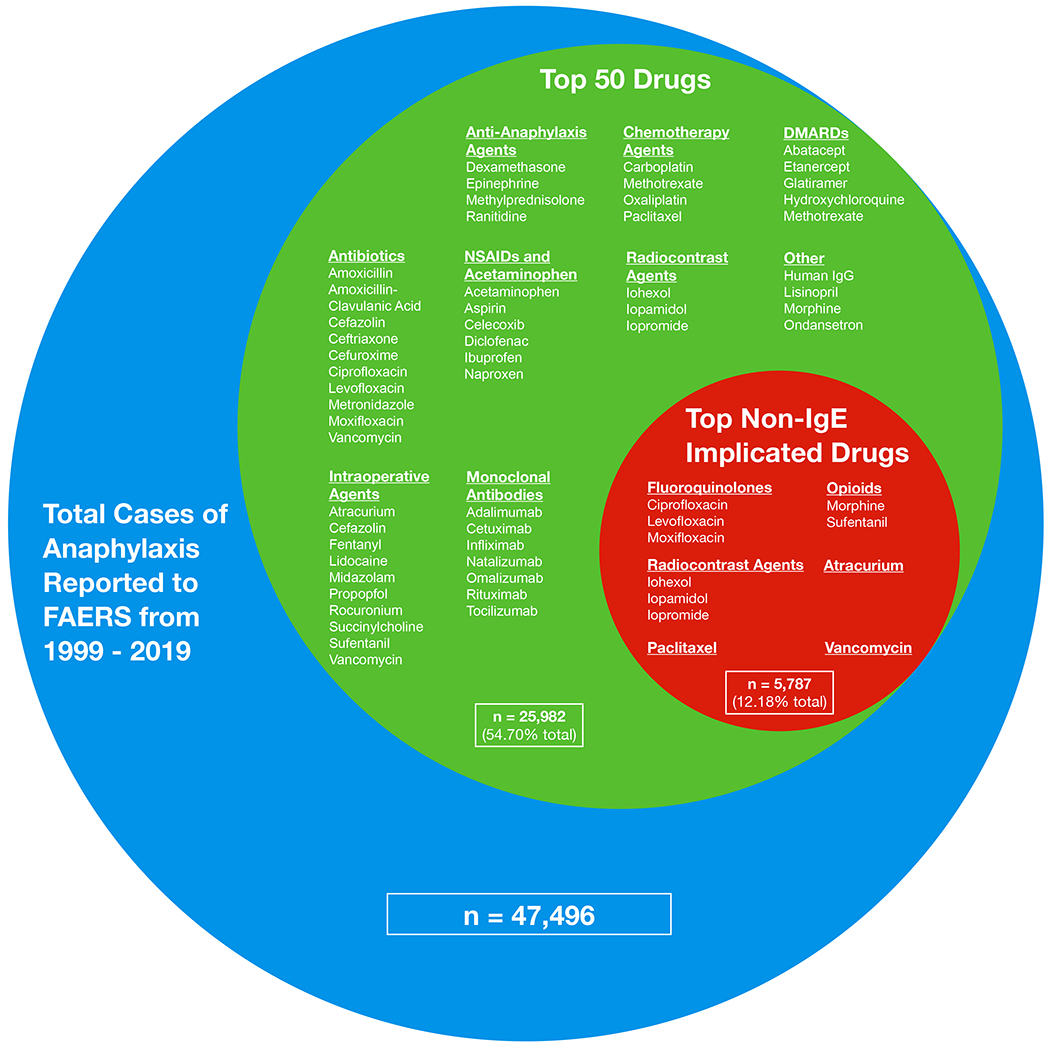
Methods: We reviewed the publicly available FAERS database from 1999 to 2019. Using search terms "anaphylactic shock" or "anaphylactic reaction" and sorting cases by generic drug names, we counted and trended reports to FAERS in which a drug was associated with anaphylaxis or anaphylaxis followed by death.
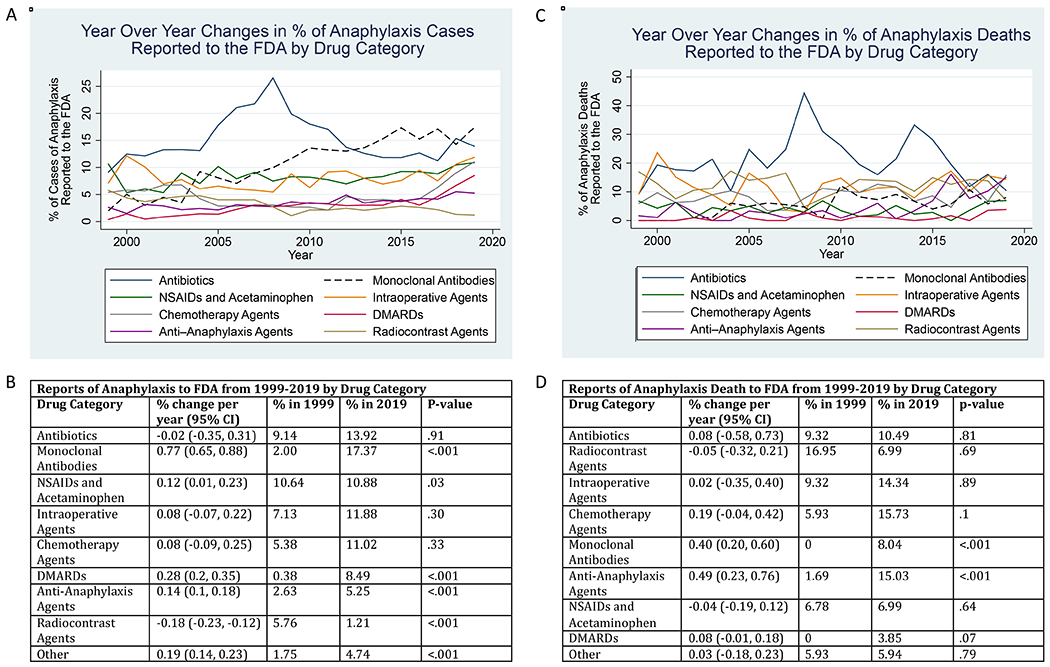
Results: From 1999 to 2019, there were 17,506,002 adverse drug events reported in FAERS, of which 47,496 (0.27%) were reported as anaphylaxis. Excluding patients without age, sex, or country data, respectively, the median age of patients in reports of anaphylaxis was 52 (interquartile range: 28), 62.71% were female, and 13,899 of 34,381 (40.43%) reports were from the United States. There were 2984 of 47,496 (6.28%) reports of anaphylaxis followed by death. Top drug classes associated with anaphylaxis in FAERS were antibiotics, monoclonal antibodies (mAbs), nonsteroidal anti-inflammatory drugs, and acetaminophen. Top drug classes associated with anaphylaxis deaths were antibiotics, radiocontrast agents, and intraoperative agents. Linear regression demonstrated reports of anaphylaxis to mAbs increasing at an average rate of 0.77% of total anaphylaxis reports per year (95% confidence interval: 0.65, 0.88) from 2.00% in 1999 to 17.37% in 2019, faster than any other drug class.
Conclusion: Antibiotics were highly reported for anaphylaxis overall and anaphylaxis followed by death. Increasing reports were noted for anaphylaxis to mAb therapies.
Keywords: Anaphylaxis; Death; Drug allergy; FAERS; FDA; Fatal.
Copyright © 2020 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Liang E, Chen L, Macy E. Adverse Reactions Associated with Penicillins, Carbapenems, Monobactams, and Clindamycin: A Retrospective Population-based Study. J Allergy Clin Immunol Pract 2020; 8:1302–13 e2. - PubMed
-
- Kowalski M, Makowska J, Blanca M, Bavbek S, Bochenek G, Bousquet J, et al. Hypersensitivity to nonsteroidal anti-inflammatory drugs (NSAIDs) - classification, diagnosis and management: review of the EAACI/ENDA(#) and GA2LEN/HANNA*. Allergy 2011; 66:818–29. - PubMed
-
- Kelso J MRGPRX2 signaling and skin test results. J Allergy Clin Immunol Pract 2020; 8:426. - PubMed
-
- Weiler C Mastocytosis, Quinolones, MRGPRX2, and Anaphylaxis. J Allergy Clin Immunol Pract 2019; 7:2091–2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
