

Higher-order connections between stereotyped subsets: implications for improved patient classification in CLL
- PMID: 32992344
- PMCID: PMC7976441
- DOI: 10.1182/blood.2020007039
Higher-order connections between stereotyped subsets: implications for improved patient classification in CLL
Abstract
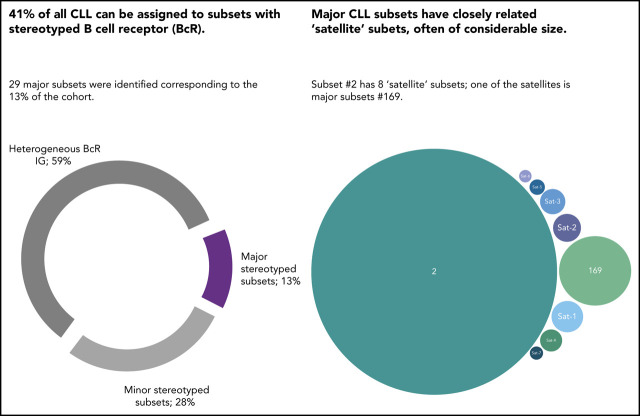
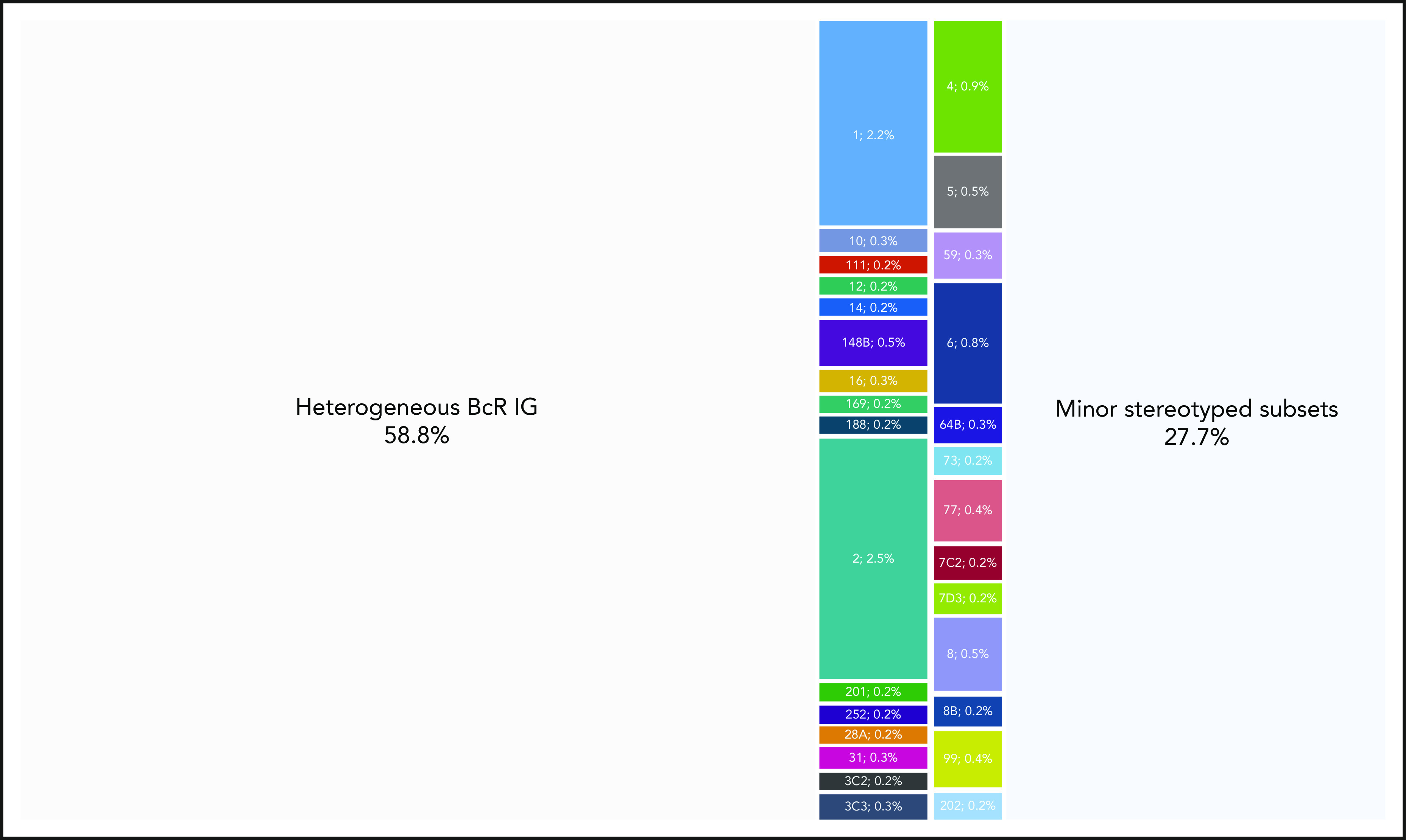
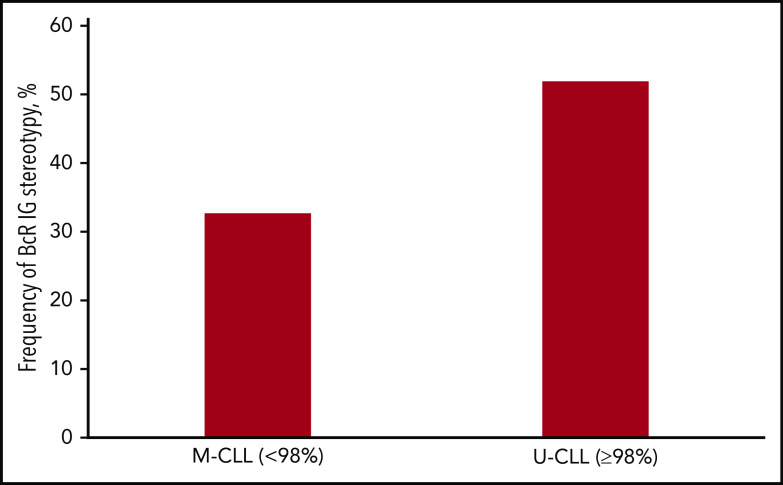
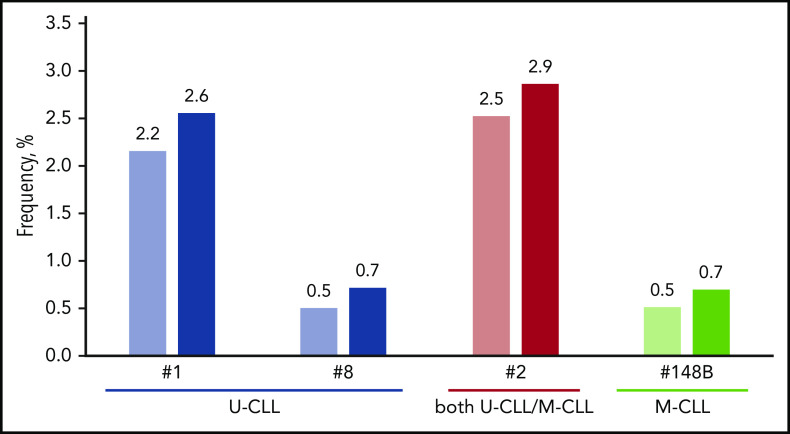
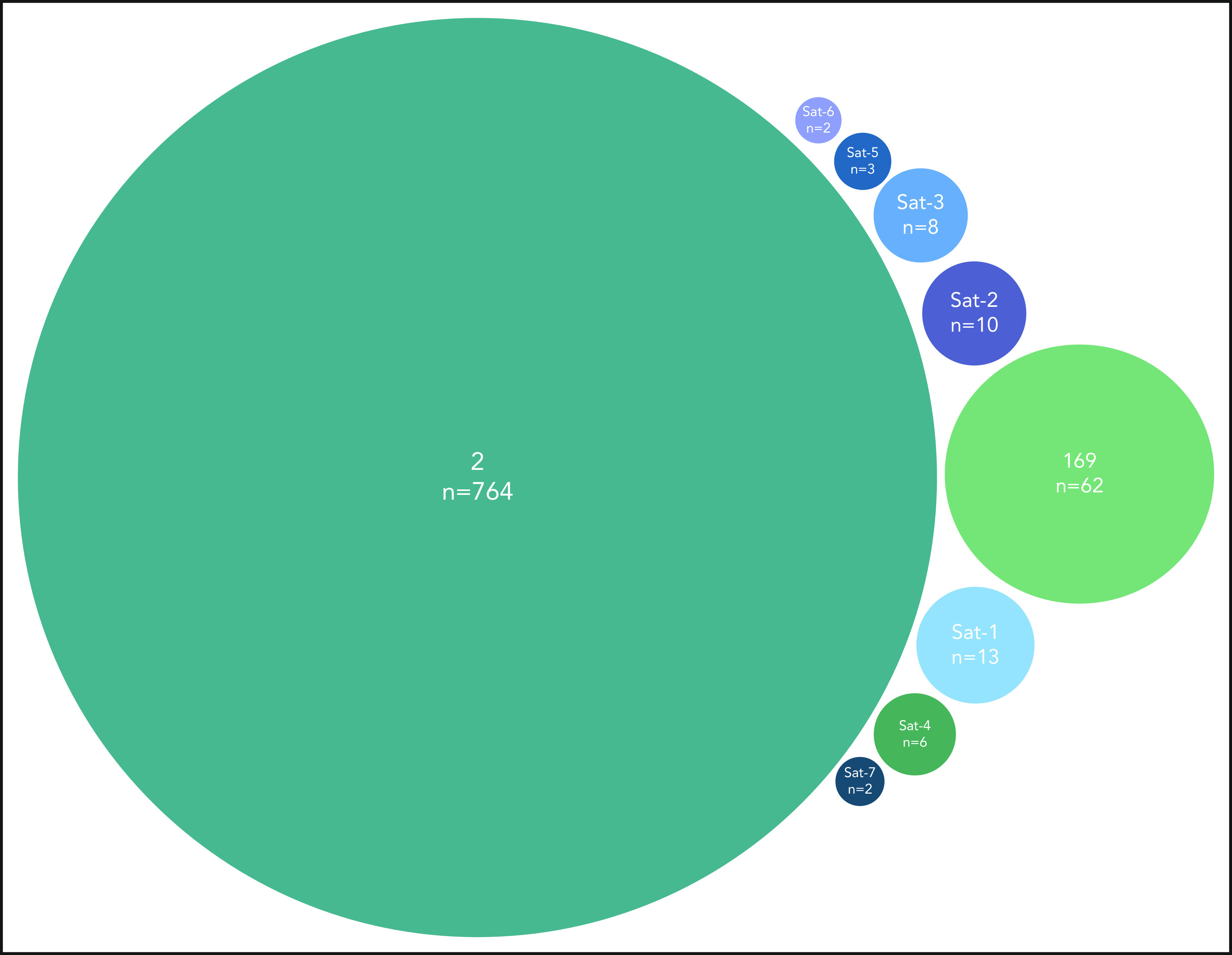
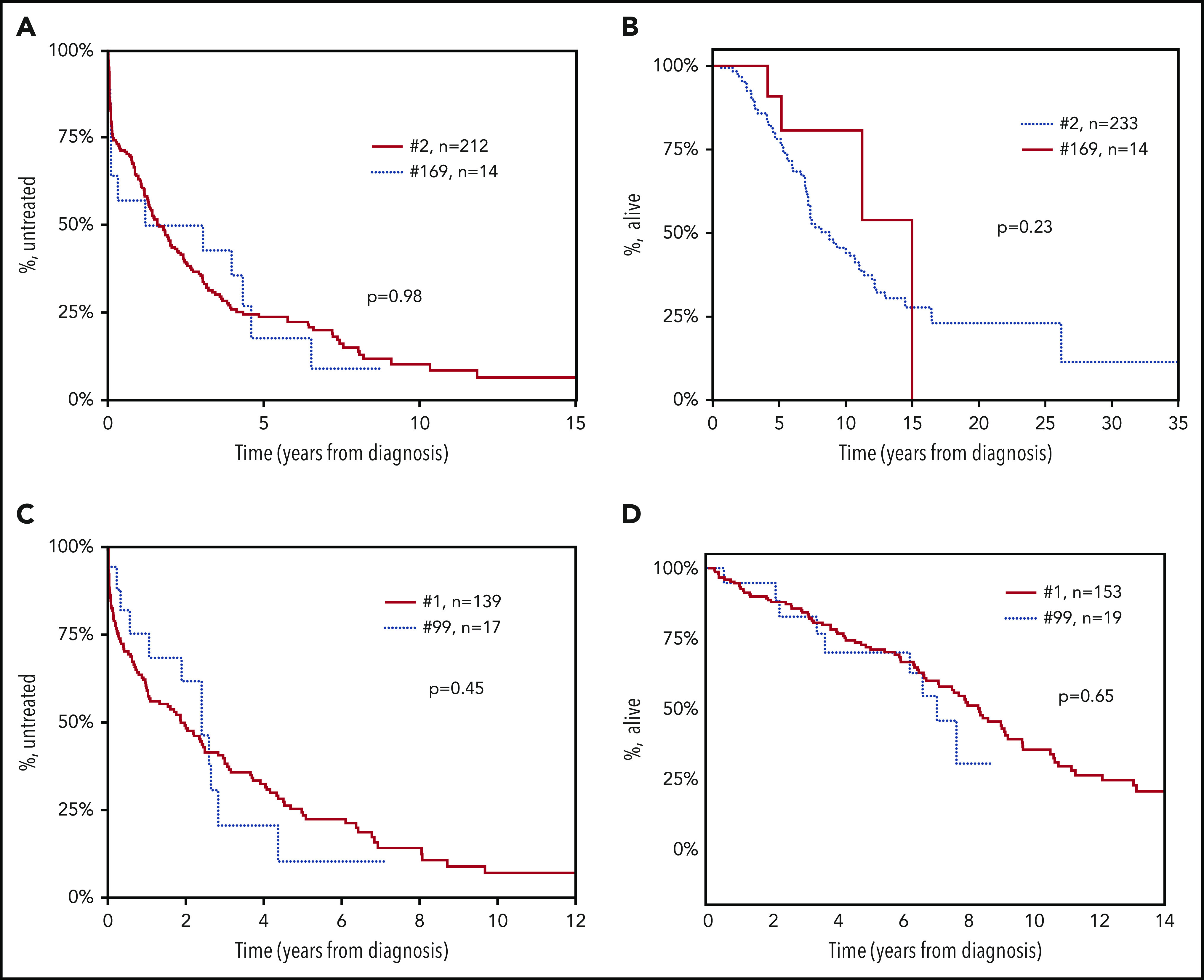
Chronic lymphocytic leukemia (CLL) is characterized by the existence of subsets of patients with (quasi)identical, stereotyped B-cell receptor (BcR) immunoglobulins. Patients in certain major stereotyped subsets often display remarkably consistent clinicobiological profiles, suggesting that the study of BcR immunoglobulin stereotypy in CLL has important implications for understanding disease pathophysiology and refining clinical decision-making. Nevertheless, several issues remain open, especially pertaining to the actual frequency of BcR immunoglobulin stereotypy and major subsets, as well as the existence of higher-order connections between individual subsets. To address these issues, we investigated clonotypic IGHV-IGHD-IGHJ gene rearrangements in a series of 29 856 patients with CLL, by far the largest series worldwide. We report that the stereotyped fraction of CLL peaks at 41% of the entire cohort and that all 19 previously identified major subsets retained their relative size and ranking, while 10 new ones emerged; overall, major stereotyped subsets had a cumulative frequency of 13.5%. Higher-level relationships were evident between subsets, particularly for major stereotyped subsets with unmutated IGHV genes (U-CLL), for which close relations with other subsets, termed "satellites," were identified. Satellite subsets accounted for 3% of the entire cohort. These results confirm our previous notion that major subsets can be robustly identified and are consistent in relative size, hence representing distinct disease variants amenable to compartmentalized research with the potential of overcoming the pronounced heterogeneity of CLL. Furthermore, the existence of satellite subsets reveals a novel aspect of repertoire restriction with implications for refined molecular classification of CLL.
© 2021 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: S.V. has received honoraria from Bayer, AstraZeneca, and Janssen; A.K. has received research funding from AbbVie, Roche/Genentech, Janssen, and AstraZeneca. D.R. has received honoraria from AbbVie, AstraZeneca, Gilead, Janssen, Verastem, and research grants from AbbVie, Gilead, Janssen, and Cellestia. S.A. has received educational grants from Johnson & Johnson, AbbVie, and Roche. K. Giannopoulos has received honoraria from AbbVie, Janssen, and Roche. L.T. has received honoraria from AbbVie, Roche, Janssen, and Shire. A.V. has received honoraria from Janssen and AbbVie. G.G. has received honoraria from AbbVie, Janssen, Sunesis, and AstraZeneca for advisory boards or speaker’s bureau services. C.N. has received research support, consultancy fees, and/or travel grants from AbbVie, Gilead, Janssen, Roche, CSL Behring, Genmab, Sunesis, and Acerta/AstraZeneca outside this work. K.F. has received honoraria from Roche and AbbVie, and Roche travel grants. S.S. has received honoraria and research support from AbbVie, AstraZeneca, Celgene, Gilead, GlaxoSmithKline, Hoffmann La-Roche, Janssen, and Novartis. R.R. has received honoraria from AbbVie, Illumina, Janssen, and Roche. P.G. has received honoraria from AbbVie, Acerta, BeiGene, Gilead, Janssen, Sunesis, and reseach funding from AbbVie, Gilead, Janssen, Novartis, and Sunesis. K.S. has received honoraria and research support from AbbVie, Janssen, AstraZeneca, and Gilead. The remaining authors declare no competing financial interests.
Figures
References
-
- Sutton LA, Rosenquist R. The complex interplay between cell-intrinsic and cell-extrinsic factors driving the evolution of chronic lymphocytic leukemia. Semin Cancer Biol. 2015;34:22-35. - PubMed
-
- Puente XS, Jares P, Campo E. Chronic lymphocytic leukemia and mantle cell lymphoma: crossroads of genetic and microenvironment interactions. Blood. 2018;131(21):2283-2296. - PubMed
-
- Jones JA, Robak T, Brown JR, et al. Efficacy and safety of idelalisib in combination with ofatumumab for previously treated chronic lymphocytic leukaemia: an open-label, randomised phase 3 trial. Lancet Haematol. 2017;4(3):e114-e126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
