

Twelve Children with Varicella Vaccine Meningitis: Neuropathogenesis of Reactivated Live Attenuated Varicella Vaccine Virus
- PMID: 32992805
- PMCID: PMC7599892
- DOI: 10.3390/v12101078
Twelve Children with Varicella Vaccine Meningitis: Neuropathogenesis of Reactivated Live Attenuated Varicella Vaccine Virus
Abstract
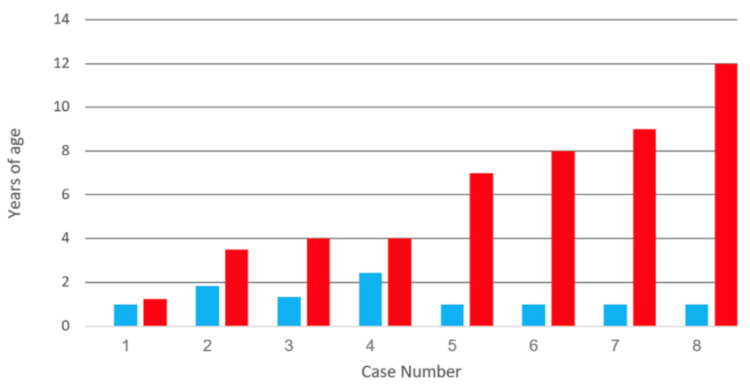
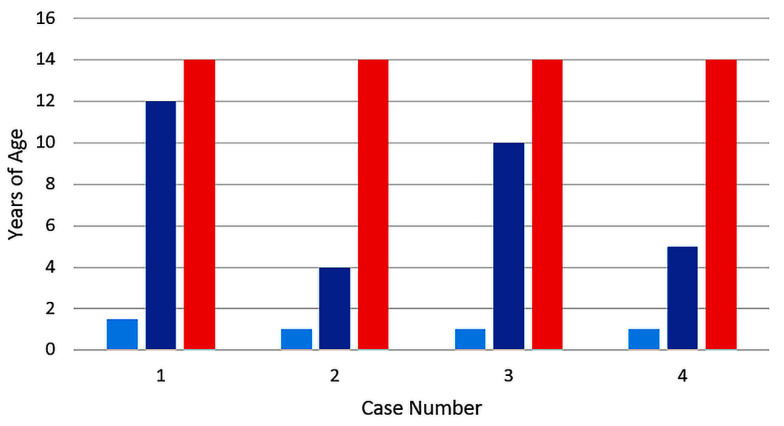
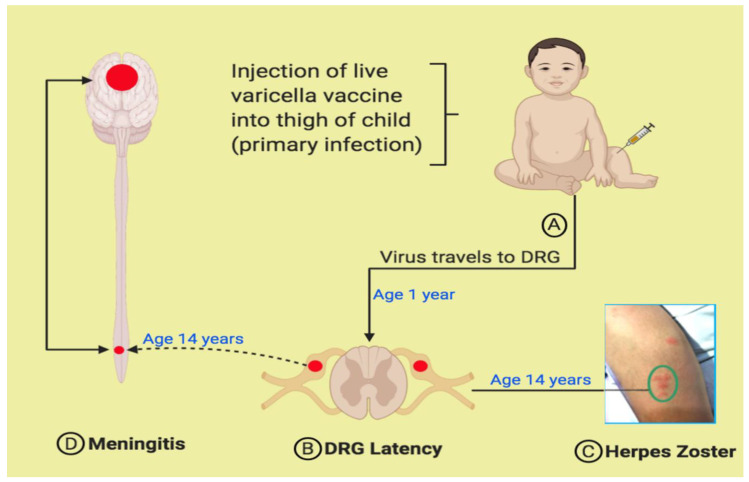
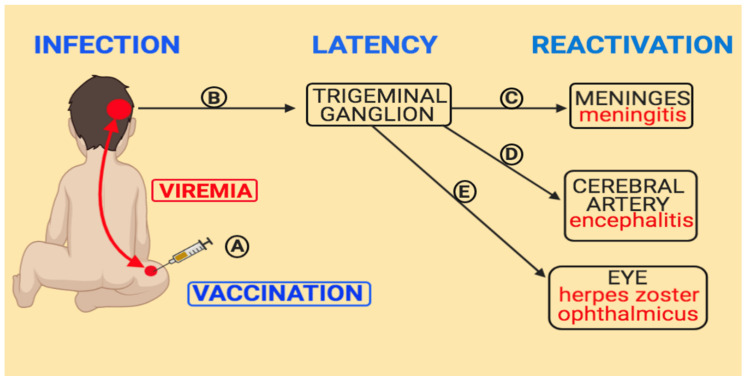
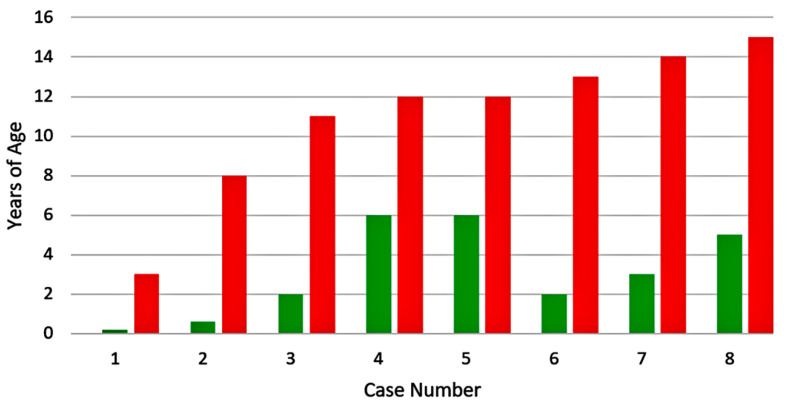
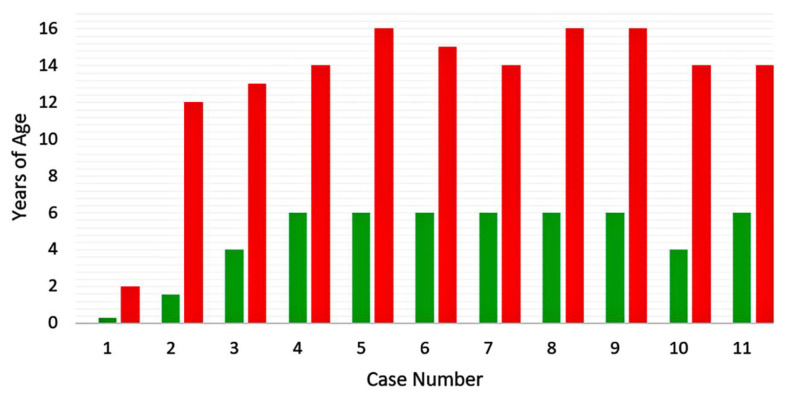
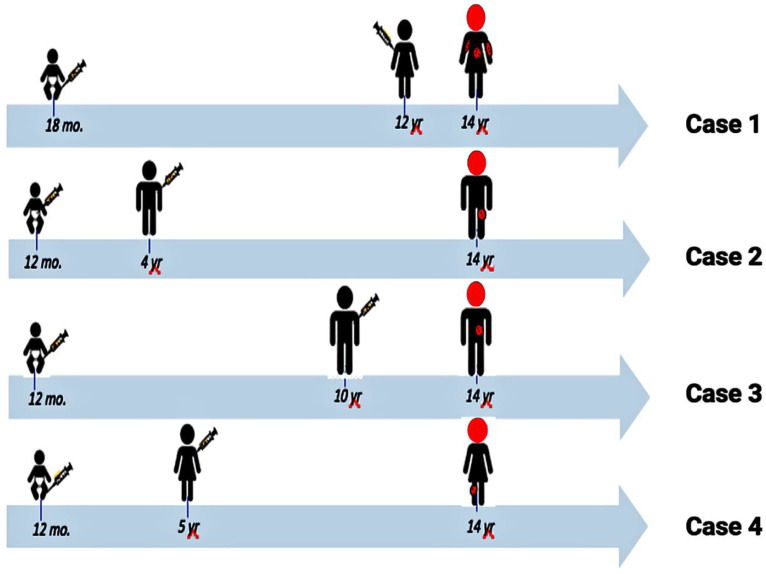
Varicella vaccine is a live attenuated varicella-zoster virus (VZV). Like its parental strain called VZV pOka, the vaccine virus vOka retains some neurotropic properties. To better understand vOka neuropathogenesis, we reassessed 12 published cases of vOka meningitis that occurred in once-immunized and twice-immunized children, all of whom had bouts of herpes zoster preceding the central nervous system infection. Eight of the 12 meningitis cases occurred in children who had received only one immunization. There was no pattern to the time interval between varicella vaccination and the onset of herpes zoster with meningitis. Four of the meningitis cases occurred in children who had received two immunizations. Since all four children were 14 years old when meningitis was diagnosed, there was a strong pattern to the interval between the first vaccination at age 1 year and onset of meningitis, namely, 13 years. Knowledge of pathogenesis requires knowledge of the location of herpes zoster; the majority of dermatomal rashes occurred at sites of primary immunization on the arm or thigh, while herpes zoster ophthalmicus was uncommon. Based on this literature review, currently there is no consensus as to the cause of varicella vaccine meningitis in twice-immunized children.
Keywords: RNA polymerase III; VZV gC; herpes vaccine; herpes zoster; latency; trigeminal ganglion; varicella-zoster virus; viral meningitis.
Conflict of interest statement
The authors declare no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Ramachandran V., Elliott S.C., Rogers K.L., Cohrs R.J., Weinberger M., Jackson W., Carpenter J.E., Grose C., Bonthius D.J. Varicella Vaccine Meningitis as a Complication of Herpes Zoster in Twice-Immunized Immunocompetent Adolescents. J. Child Neurol. 2020:883073820938597. doi: 10.1177/0883073820938597. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
