

Factors contributing to diagnostic delay of Caroli syndrome: a single-center, retrospective study
- PMID: 32993513
- PMCID: PMC7523362
- DOI: 10.1186/s12876-020-01442-5
Factors contributing to diagnostic delay of Caroli syndrome: a single-center, retrospective study
Abstract
Background: Caroli syndrome (CS) is a rare congenital disorder without pathognomonic clinical symptoms or laboratory findings; therefore, the diagnosis is often delayed. The objective of this study was to investigate the diagnostic delay and associated risk factors in CS patients.
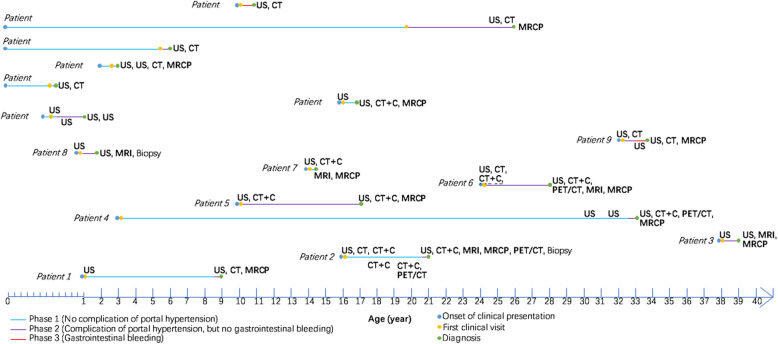
Methods: This was a retrospective analysis of 16 CS patients admitted to a single tertiary medical center on mainland China. The diagnostic timelines of CS patients were reviewed to demonstrate the initial findings of CS at diagnosis, the risk factors associated with diagnostic delay, and potential clues leading to early diagnosis.
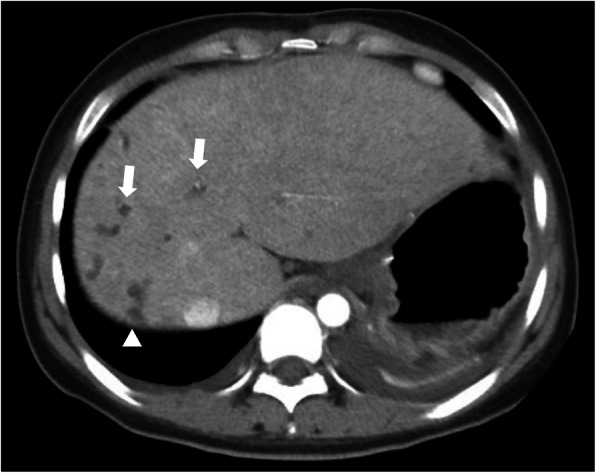
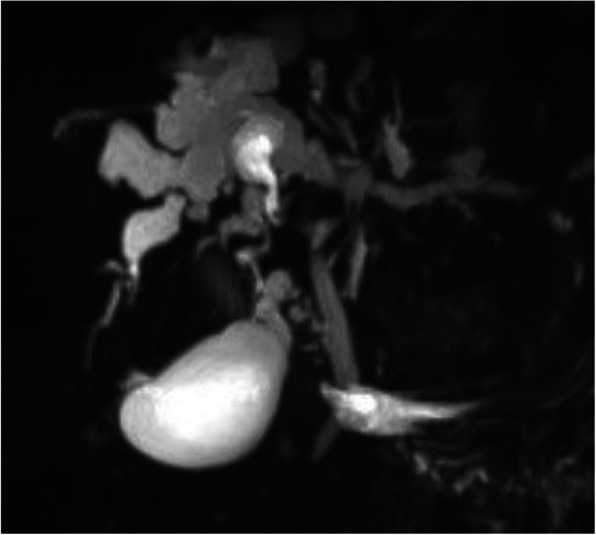
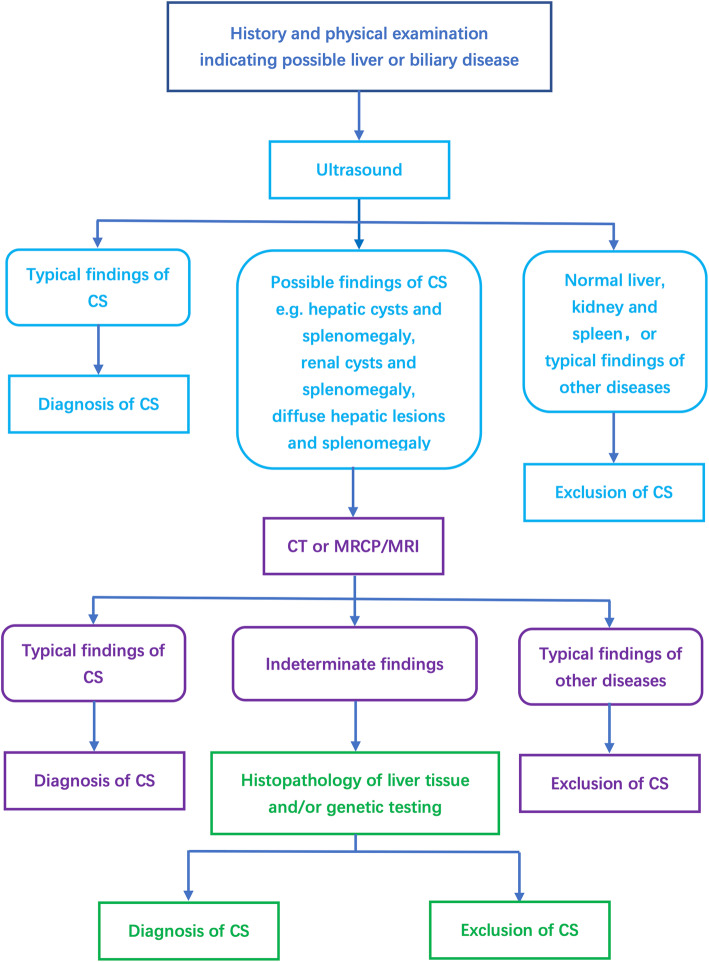
Results: The median diagnostic delay was 1.75 years (range: 1 month to 29 years, interquartile range: 6.2 years) in 16 enrolled CS patients. Sex, age, and initial symptoms were not associated with diagnostic delay. 87.5% of CS patients were diagnosed by imaging, and the accuracies of ultrasonography, computed tomography (CT), and magnetic resonance cholangiopancreatography were 25, 69.2, and 83.3%, respectively. The median diagnostic delays for patients with or without CT performed at the first hospital visited according to physician and radiologist suspicion of the diagnosis were 7.4 months and 6 years, respectively (p = 0.021). Hepatic cysts with splenomegaly were detected by ultrasound in over half of CS patients.
Conclusions: The majority of CS patients were not diagnosed until complications of portal hypertension had already developed. Recognition and early suspicion of the disease were important factors influencing diagnostic delay of CS. Hepatic cysts plus splenomegaly detected by US might raise the clinical suspicion to include CS in the differential diagnosis.
Keywords: Caroli syndrome; Diagnosis; Imaging.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
