

Quantifying the direct secondary health care cost of seasonal influenza in England
- PMID: 32993588
- PMCID: PMC7526100
- DOI: 10.1186/s12889-020-09553-0
Quantifying the direct secondary health care cost of seasonal influenza in England
Abstract
Background: The winter pressure often experienced by NHS hospitals in England is considerably contributed to by severe cases of seasonal influenza resulting in hospitalisation. The prevention planning and commissioning of the influenza vaccination programme in the UK does not always involve those who control the hospital budget. The objective of this study was to describe the direct medical costs of secondary care influenza-related hospital admissions across different age groups in England during two consecutive influenza seasons.
Methods: The number of hospital admissions, length of stay, and associated costs were quantified as well as determining the primary costs of influenza-related hospitalisations. Data were extracted from the Hospital Episode Statistics (HES) database between September 2017 to March 2018 and September 2018 to March 2019 in order to incorporate the annual influenza seasons. The use of international classification of disease (ICD)-10 codes were used to identify relevant influenza hospitalisations. Healthcare Resource Group (HRG) codes were used to determine the costs of influenza-related hospitalisations.
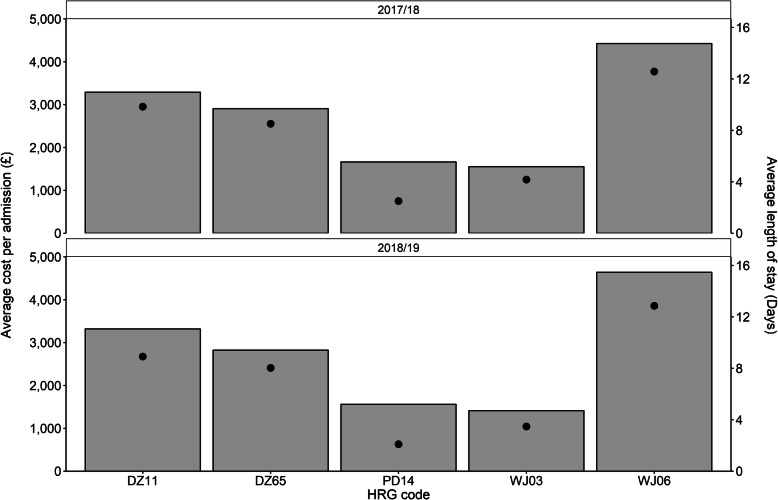
Results: During the 2017/18 and 2018/19 seasons there were 46,215 and 39,670 influenza-related hospital admissions respectively. This resulted in a hospital cost of £128,153,810 and £99,565,310 across both seasons. Results showed that those in the 65+ year group were associated with the highest hospitalisation costs and proportion of in-hospital deaths. In both influenza seasons, the HRG code WJ06 (Sepsis without Interventions) was found to be associated with the longest average length of stay and cost per admission, whereas PD14 (Paediatric Lower Respiratory Tract Disorders without Acute Bronchiolitis) had the shortest length of stay.
Conclusion: This study has shown that influenza-related hospital admissions had a considerable impact on the secondary healthcare system during the 2017/18 and 2018/19 influenza seasons, before taking into account its impact on primary health care.
Keywords: Burden of illness; HES; Hospital episode statistics; Hospitalisation; Immunisation; Influenza; Secondary healthcare; Vaccination.
Conflict of interest statement
IG, CD and SC are employees of Sanofi Pasteur.
Figures

References
-
- Iuliano AD, Roguski KM, Chang HH, Muscatello DJ, Palekar R, Tempia S, Cohen C, Gran JM, Schanzer D, Cowling BJ, et al. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet. 2018;391(10127):1285–1300. doi: 10.1016/S0140-6736(17)33293-2. - DOI - PMC - PubMed
-
- Public Health England. Surveillance of influenza and other respiratory viruses in the UK: winter 2017 to 2018. London: Public Health England; 2018.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
