

The Amyloidosis Forum: a public private partnership to advance drug development in AL amyloidosis
- PMID: 32993758
- PMCID: PMC7523334
- DOI: 10.1186/s13023-020-01525-2
The Amyloidosis Forum: a public private partnership to advance drug development in AL amyloidosis
Abstract
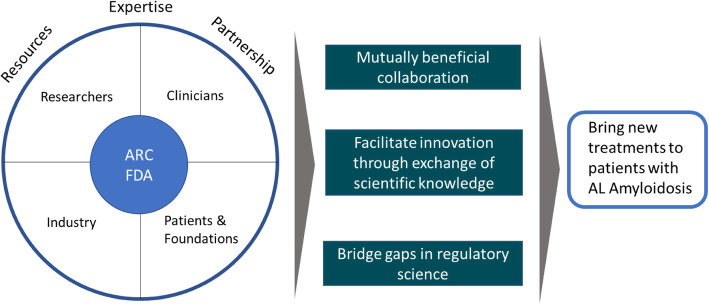
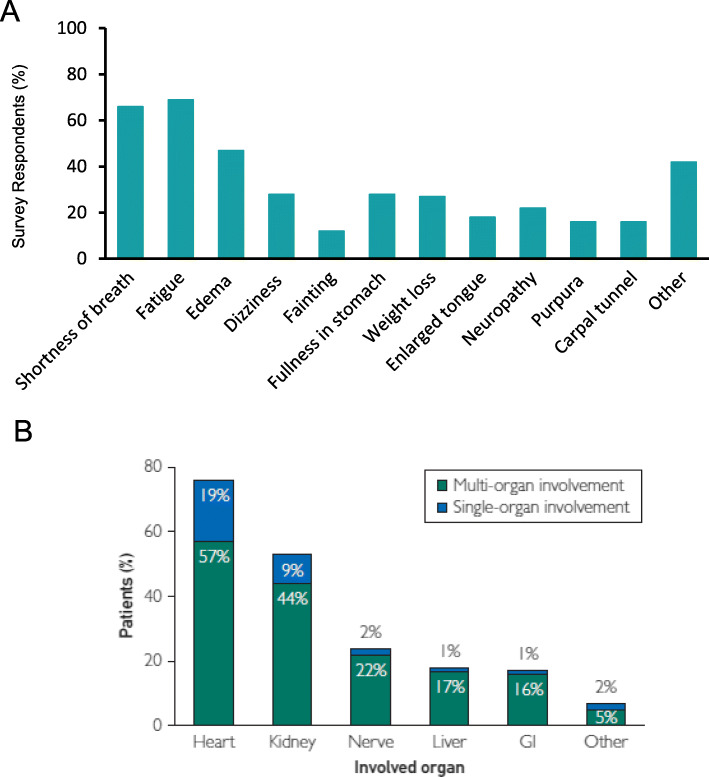
Background: Immunoglobulin light chain (AL) amyloidosis is a rare, multi-systemic disorder characterized by two disease processes: an underlying plasma cell dyscrasia that provides the source of pathologic light chains, and the resulting organ dysfunction caused by deposition of amyloid light chain fibrils. There are no FDA approved treatments for AL amyloidosis; regimens developed for multiple myeloma are used off-label to treat the plasma cell disorder and no therapies are directed at organ deposition. Thus, an unmet medical need persists despite advances in disease management. A public-private partnership was recently formed between the Amyloidosis Research Consortium (ARC) and the US Food and Drug Administration (FDA) to bridge scientific gaps in drug development for the treatment of AL amyloidosis.
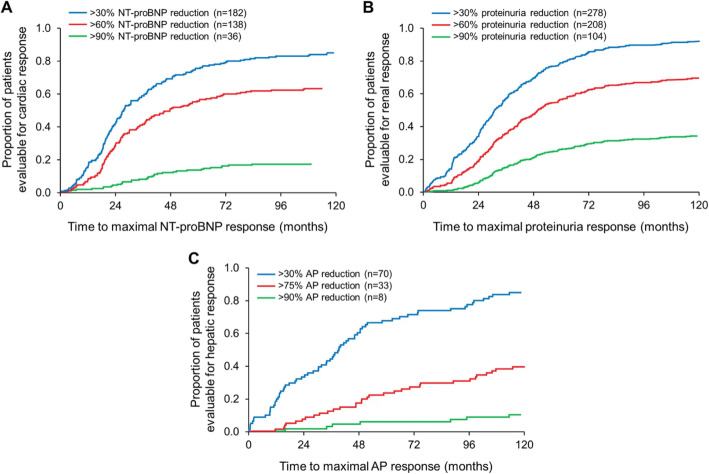
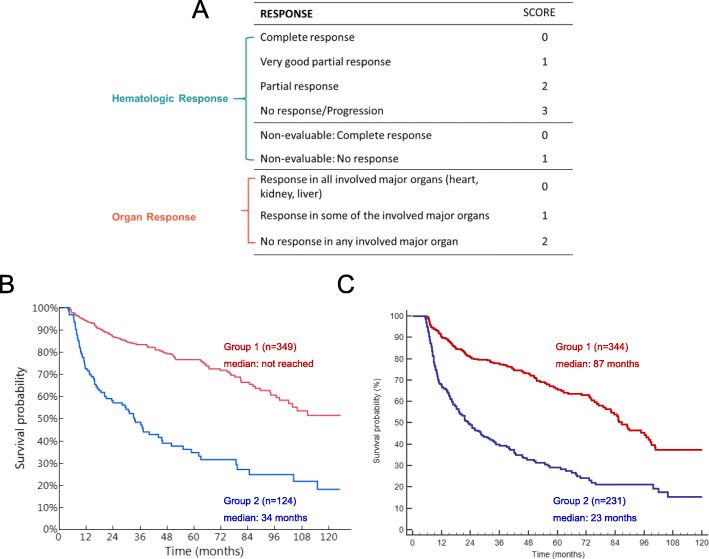
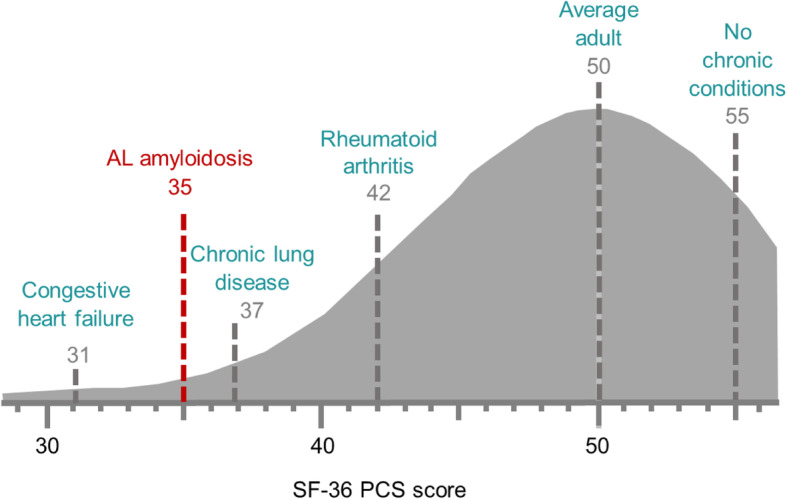
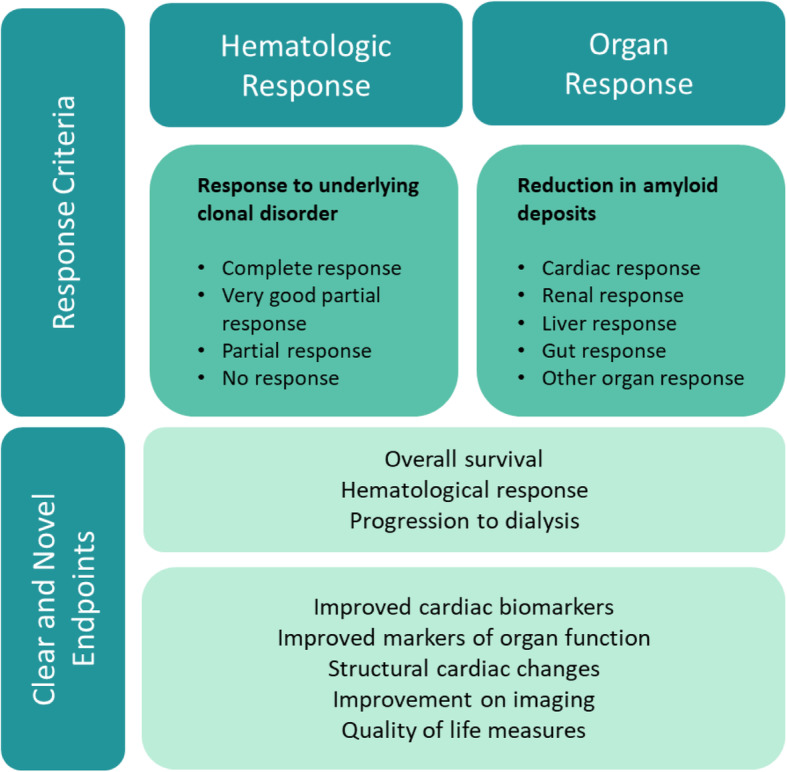
Main body: The inaugural Amyloidosis Forum was convened at FDA on 12 November 2019 and led by a multidisciplinary panel of physicians, health outcomes professionals, and representatives from the FDA, ARC, and pharmaceutical companies. Patients provided important perspectives on the pathway to diagnosis, challenges of rigorous treatment, and the burden of disease. The panel reviewed the epidemiology, pathobiology, and clinical features of AL amyloidosis. Hematologic characteristics, staging systems, and response criteria were examined with clear consensus that a "deep response" to plasma cell-directed treatments was critical to overall survival. Emphasis was placed on the heterogeneous clinical phenotypes of AL amyloidosis, including cardiovascular, renal, neurological, and gastrointestinal system manifestations that contribute to morbidity and/or mortality, but render challenges to clinical trial endpoint selection. FDA representatives discussed regulatory perspectives regarding demonstration of clinical benefits of investigational therapies in the context of a rare disease with multi-systemic manifestations. The panel also highlighted the potential importance of well-designed health-related quality of life instruments, quantification of system organ effects, the potential of advanced imaging technologies, and survival prediction models.
Conclusions: The Amyloidosis Forum identified a clear need for novel trial designs that are scientifically rigorous, feasible, and incorporate clinically meaningful endpoints based on an understanding of the natural history of the disease in an evolving therapeutic landscape. Future forums will delve into these issues and seek to include participation from additional stakeholders.
Keywords: AL amyloidosis; Drug development; Light-chain amyloidosis; Primary amyloidosis.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Muchtar E, Gertz MA, Kyle RA, Lacy MQ, Dingli D, Leung N, et al. A modern primer on light chain amyloidosis in 592 patients with mass spectrometry-verified typing. Mayo Clin Proc. 2019;94(3):472–483. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
