

Confronting power in low places: historical analysis of medical dominance and role-boundary negotiation between health professions in Nigeria
- PMID: 32994230
- PMCID: PMC7526320
- DOI: 10.1136/bmjgh-2020-003349
Confronting power in low places: historical analysis of medical dominance and role-boundary negotiation between health professions in Nigeria
Abstract
Introduction: Interprofessional interaction is intrinsic to health service delivery and forms the basis of task-shifting and task-sharing policies to address human resources for health challenges. But while interprofessional interaction can be collaborative, professional hierarchies and discipline-specific patterns of socialisation can result in unhealthy rivalry and conflicts which disrupt health system functioning. A better understanding of interprofessional dynamics is necessary to avoid such negative consequences. We, therefore, conducted a historical analysis of interprofessional interactions and role-boundary negotiations between health professions in Nigeria.
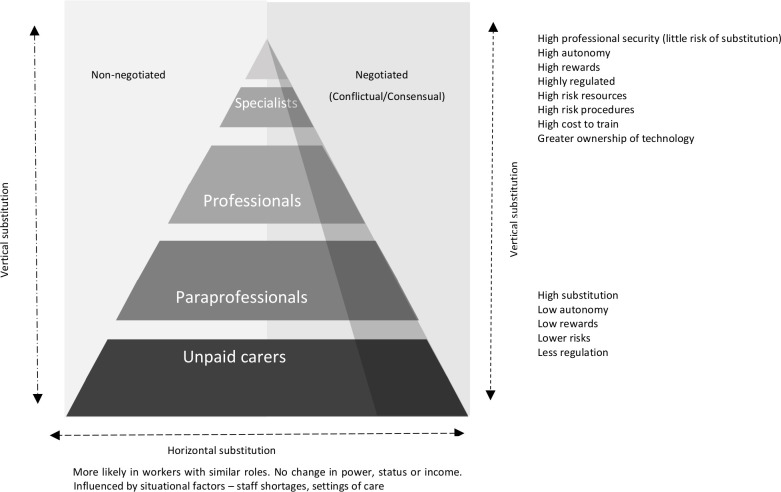
Methods: We conducted a review of both published and grey literature to provide historical accounts and enable policy tracing of reforms related to interprofessional interactions. We used Nancarrow and Borthwick's typology for thematic analysis and used medical dominance and negotiated order theories to offer explanations of the conditions that facilitated or constrained interprofessional collaboration.
Results: Despite an overall context of medical dominance, we found evidence of professional power changes (dynamics) and role-boundary shifts between health professions. These shifts occurred in different directions, but shifts between professions that are at different power gradients were more likely to be non-negotiable or conflictual. Conditions that facilitated consensual role-boundary shifts included the feasibility of simultaneous upward expansion of roles for all professions and the extent to which the delegating profession was in charge of role delegation. While the introduction of new medical diagnostic technology opened up occupational vacancies which facilitated consensual role-boundary change in some cases, it constrained professional collaboration in others.
Conclusions: Health workforce governance can contribute to better functioning of health systems and voiding dysfunctional interprofessional relations if the human resource for health interventions are informed by contextual understanding (informed by comparative institutional and health systems research) of conditions that facilitate or constrain effective interprofessional collaboration.
Keywords: health policies and all other topics; health services research; health systems.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Scheffler R, Cometto G, Tulenko K, et al. . Health workforce requirements for universal health coverage and the sustainable development goals. Geneva: World Health Organization, 2016. https://apps.who.int/iris/bitstream/handle/10665/250330/9789241511407-en...
-
- van GE, Schäfer W, Kroneman M. Managed competition in the Netherlands: an example for others? Eurohealth 2010;16:23–6.
-
- Boyce RA. Health sector reform and professional power, autonomy and culture: the case of Australian allied health professions : Concepts of care. Developments in health & social welfare. London, England: Edward Arnold, 1997: 74–88. https://www.researchgate.net/publication/45165981_Health_sector_reform_a...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources