

Guidance for the assessment and management of prostate cancer treatment-induced bone loss. A consensus position statement from an expert group
- PMID: 32995252
- PMCID: PMC7516275
- DOI: 10.1016/j.jbo.2020.100311
Guidance for the assessment and management of prostate cancer treatment-induced bone loss. A consensus position statement from an expert group
Abstract
Context and objective: Incidence of prostate cancer (PC) is increasing, but androgen deprivation therapy (ADT) and other therapies are substantially improving survival. In this context, careful consideration of skeletal health is required to reduce the risk of treatment-related fragility fractures and their associated morbidity and mortality. This risk is currently not well-managed. ADT causes significant loss of bone mineral density (BMD). In the metastatic setting, systemic treatments (e.g. chemotherapy, abiraterone, enzalutamide) are used alongside ADT and may require concomitant glucocorticoids. Both ADT and glucocorticoids pose significant challenges to skeletal health in a population of patients already likely to have ongoing age-related bone loss and/or comorbid conditions. Current PC guidelines lack specific recommendations for optimising bone health. This guidance presents evidence for assessment and management of bone health in this population, with specific recommendations for clinical practitioners in day-to-day PC management.
Methods: Structured meetings of key opinion leaders were integrated with a systematic literature review. Input and endorsement was sought from patients, nursing representatives and specialist societies.
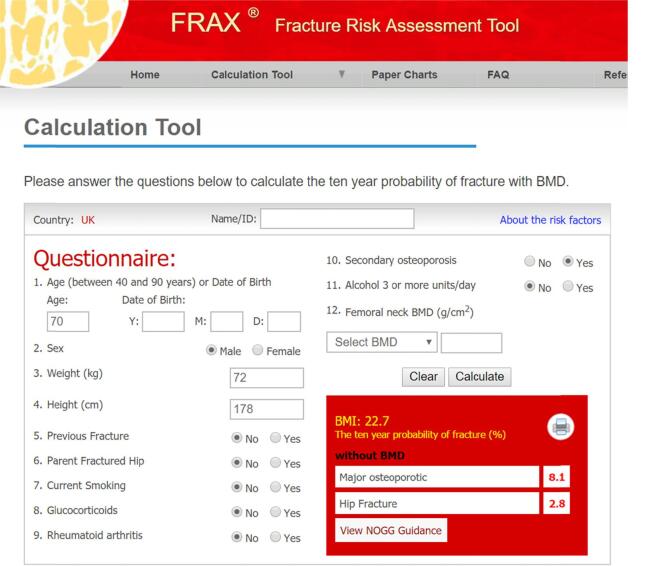
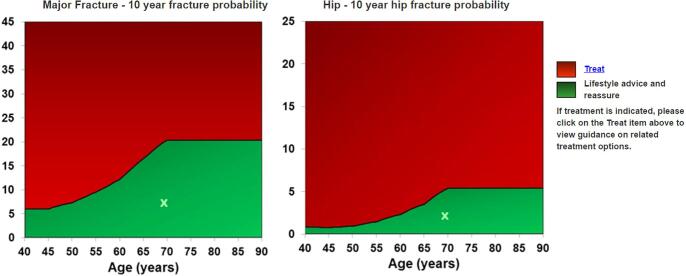
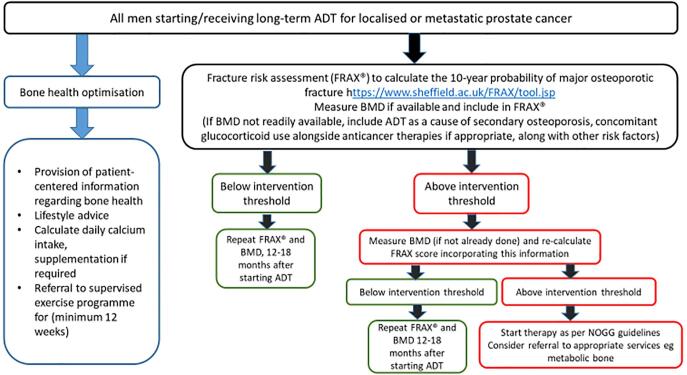
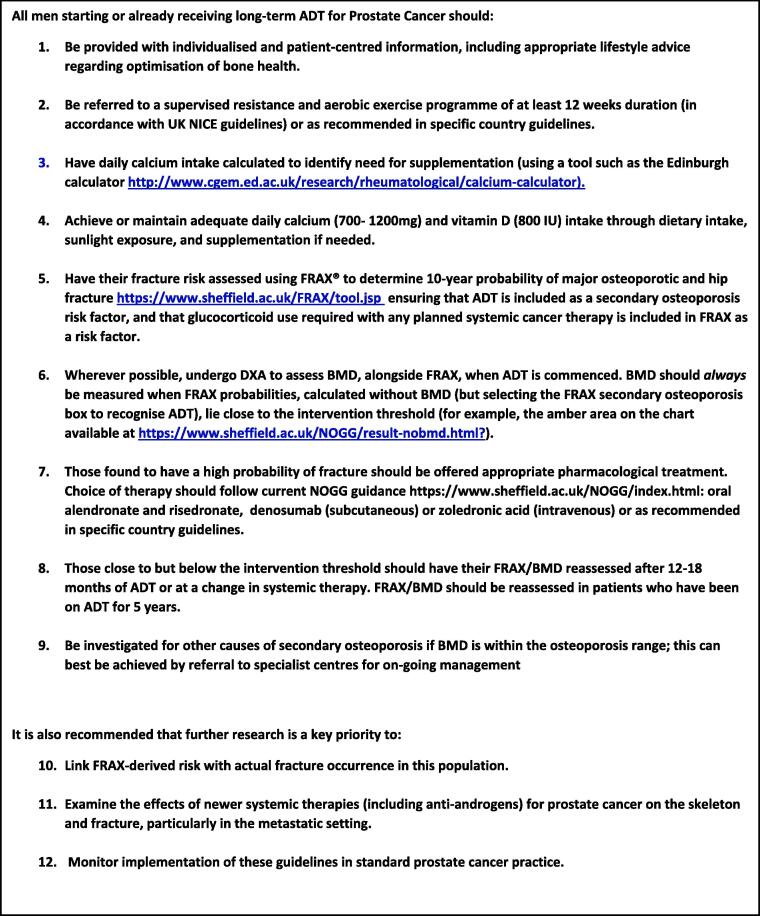
Summary of guidance: All men starting or continuing long-term ADT should receive lifestyle advice regarding bone health. Calcium/vitamin D supplementation should be offered if required. Fracture risk should be calculated (using the FRAX® tool), with BMD assessment included where feasible. BMD should always be assessed where fracture risk calculated using FRAX® alone is close to the intervention threshold. Intervention should be provided if indicated by local or national guidelines e.g. UK National Osteoporosis Guideline Group (NOGG) thresholds. Men requiring bone protection therapy should be further assessed (e.g. renal function), with referral to specialist centres if available and offered appropriate treatment to reduce fracture risk. Those near to, but below an intervention threshold, and patients going on to additional systemic therapies (particularly those requiring glucocorticoids), should have FRAX® (including BMD) repeated after 12-18 months.
Patient summary: Modern treatments for prostate cancer have led to significant improvements in survival and quality of life. However, some of these treatments may lead to weakening of patient's bones with risk of fracture and it is therefore important to monitor patients' bone health and provide bone protection where needed. This paper provides specific guidance to clinical teams, based on the most recent research evidence, to ensure optimal bone health in their patients.
Keywords: Fracture risk; Guidelines; Osteoporosis; Prostate cancer; Skeletal health.
© 2020 Published by Elsevier GmbH.
Figures
References
-
- Cancer research UK mortality statistics. Available from: http://www.cancerresearchuk.org/health-professional/cancer-statistics/st....
-
- Cancer Research UK. Cancer statistics. 2013 Available from: http://www.cancerresearchuk.org/health-professional/cancer-statistics/st....
-
- Thorstenson A., Bratt O., Akre O. Incidence of fractures causing hospitalisation in prostate cancer patients: Results from the population-based PCBaSe Sweden. Eur. J. Cancer. 2012;48:1672–1681. - PubMed
-
- Smith M., Parker C., Saad F., Miller K., Tombal B., Ng Q.S. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20:408–419. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
