

Approach to the patient with acute severe autoimmune hepatitis
- PMID: 32995712
- PMCID: PMC7509236
- DOI: 10.1016/j.jhepr.2020.100149
Approach to the patient with acute severe autoimmune hepatitis
Abstract
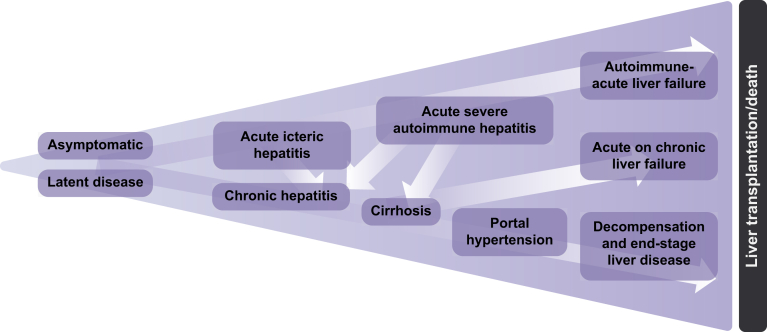
Autoimmune hepatitis is associated with varied clinical presentations and natural history, as well as somewhat unpredictable treatment responses. Understanding how to stratify patients who require further escalation of therapy will help clinicians manage these patients. The presentation of acute severe autoimmune hepatitis (AS-AIH) is relatively uncommon, although its prevalence is potentially greater than currently perceived. Previous studies consist of small retrospective single-centre series and are not directly comparable due to the diversity of presentations, disease definitions and non-standardised treatment regimens. We define AS-AIH as those who present acutely with AIH and are icteric with an international normalised ratio ≥1.5 and no evidence of hepatic encephalopathy. Those with hepatic encephalopathy should be defined as having AS-AIH with acute liver failure. In this review, we provide a structured practical approach for diagnosing and managing this unique group of patients.
Keywords: ACLF, acute-on-chronic liver failure; AIH, autoimmune hepatitis; ALF, acute liver failure; ALI, acute liver injury; ALT, alanine aminotransferase; ANA, anti-nuclear antibody; AS-AIH, acute severe autoimmune hepatitis; ASMA, anti-smooth muscle antibody; AST, aspartate aminotransferase; AUROC, analysis of area under the receiver operator characteristic curve; Acute liver failure; Acute severe presentation; Autoimmune hepatitis; CT, computed tomography; Corticosteroids; DILI, drug-induced liver injury; EBV, Epstein-Barr virus; HE, hepatic encephalopathy; HLA, human leukocyte antigen; IAIHG, International Autoimmune Hepatitis Group; INR, international normalised ratio; LT, liver transplantation; Liver transplantation; MELD, model for end-stage liver disease; MELD-Na, model for end-stage liver disease-sodium; MHN, massive hepatic necrosis; NAC, N-acetylcysteine; PT, prothrombin time; UKELD, United Kingdom end-stage liver disease; USALF, United States Acute Liver Failure; anti-LC-1, anti-liver cytosol-1; anti-LKM, anti-liver kidney microsomal; anti-SLA/LP, anti-soluble liver antigen/liver pancreas.
© 2020 The Authors.
Conflict of interest statement
The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
-
- Lohse A.W., Chazouillères O., Dalekos G., Drenth J., Heneghan M., Hofer H. EASL clinical practice guidelines: autoimmune hepatitis. J Hepatol. 2015;63(4):971–1004. - PubMed
-
- Mack C.L., Adams D., Assis D.N., Kerkar N., Manns M.P., Mayo M.J. Diagnosis and management of autoimmune hepatitis in adults and children: 2019 practice guidance and guidelines from the American Association for the Study of Liver Diseases. Hepatology. 2019;72(2):671–722. - PubMed
-
- Trey C., Davidson C.S. The management of fulminant hepatic failure. Prog Liver Dis. 1970;3:282–298. - PubMed
-
- Williams R., Schalm S.W., O'Grady J.G. Acute liver failure: redefining the syndromes. Lancet. 1993;342(8866):273–275. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
