

In-Hospital Postoperative Mortality Rates for Selected Procedures in Tanzania's Lake Zone
- PMID: 32995932
- PMCID: PMC7752880
- DOI: 10.1007/s00268-020-05802-w
In-Hospital Postoperative Mortality Rates for Selected Procedures in Tanzania's Lake Zone
Abstract
Background: Postoperative mortality rate is one of six surgical indicators identified by the Lancet Commission on Global Surgery for monitoring access to high-quality surgical care. The primary aim of this study was to measure the postoperative mortality rate in Tanzania's Lake Zone to provide a baseline for surgical strengthening efforts. The secondary aim was to measure the effect of Safe Surgery 2020, a multi-component intervention to improve surgical quality, on postoperative mortality after 10 months.
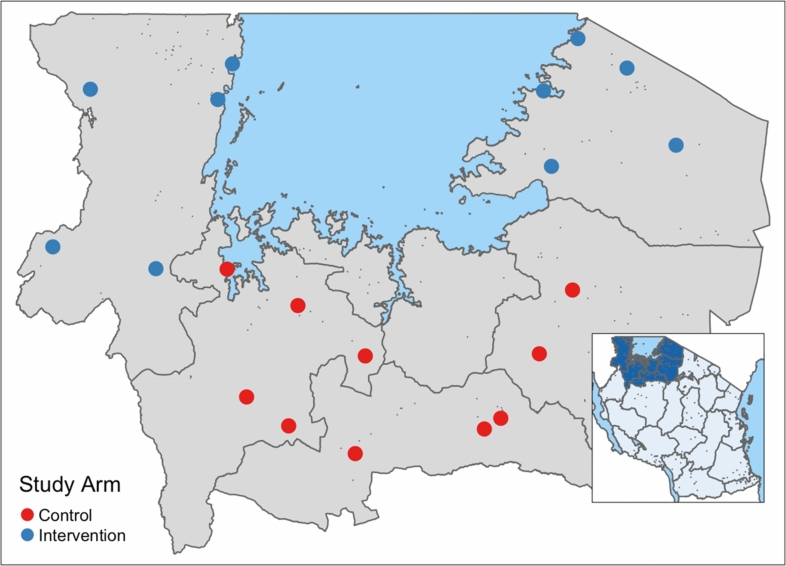
Methods: We prospectively collected data on postoperative mortality from 20 health centers, district hospitals, and regional hospitals in Tanzania's Lake Zone over two time periods: pre-intervention (February to April 2018) and post-intervention (March to May 2019). We analyzed postoperative mortality rates by procedure type. We used logistic regression to determine the impact of Safe Surgery 2020 on postoperative mortality.
Results: The overall average in-hospital non-obstetric postoperative mortality rate for all surgery procedures was 2.62%. The postoperative mortality rates for laparotomy were 3.92% and for cesarean delivery was 0.24%. Logistic regression demonstrated no difference in the postoperative mortality rate after the Safe Surgery 2020 intervention.
Conclusions: Our results inform national surgical planning in Tanzania by providing a sub-national baseline estimate of postoperative mortality rates for multiple surgical procedures and serve as a basis from which to measure the impact of future surgical quality interventions. Our study showed no improvement in postoperative mortality after implementation of Safe Surgery 2020, possibly due to low power to detect change.
Conflict of interest statement
The Program in Global Surgery and Social Change, Dalberg Advisors, Jhpiego, and Assist International receive funding from the GE Foundation for the Safe Surgery 2020 project. Shehnaz Alidina, Isabelle Citron, Erastus Maina, Gopal Menon, Cheri Reynolds, Chris Strader, John Varallo, Isabelle Citron, Adelina Mazhiqi, Meaghan Sydlowski, Taylor Wurdeman, and John G. Meara had financial support from GE Foundation for the submitted work. David Barash is employed by GE Foundation, which funded this work. John Varallo declares financial support from ELMA Philanthropies. Fabian Massaga reports receiving a Jhpiego FAA grant. John G. Meara declares support from the Kletjian Foundation and the Ronda Stryker and William Johnston Foundation. Ntuli Kapologwe and Sarah Maongezi have nothing to declare. The authors have had no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
The Value of Reporting Perioperative Mortality Rates (POMR).World J Surg. 2021 Jan;45(1):50-52. doi: 10.1007/s00268-020-05804-8. Epub 2020 Oct 6. World J Surg. 2021. PMID: 33025155 No abstract available.
References
-
- Bickler SN, Weiser TG, Kassebaum N, et al. Global burden of surgical conditions. In: Debas HT, Donkor P, Gawande A, Jamison DT, Kruk ME, Mock CN, et al., editors. Essential surgery: disease control priorities, 3 Ed (vol 1) Washington (DC): The World Bank; 2015. p. 25.
-
- Jauniaux E, Grobman WA. Caesarean section: Introduction to the ‘World’s No. 1’ surgical procedure. In: Sathya D, editor. Textbook of caesarean section. Oxford: Oxford University Press; 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
