

Repository Corticotropin Injection for Persistently Active Systemic Lupus Erythematosus: Results from a Phase 4, Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial
- PMID: 32996096
- PMCID: PMC7695765
- DOI: 10.1007/s40744-020-00236-1
Repository Corticotropin Injection for Persistently Active Systemic Lupus Erythematosus: Results from a Phase 4, Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial
Erratum in
-
Correction to: Repository Corticotropin Injection for Persistently Active Systemic Lupus Erythematosus: Results from a Phase 4, Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial.Rheumatol Ther. 2021 Dec;8(4):1915. doi: 10.1007/s40744-021-00353-5. Rheumatol Ther. 2021. PMID: 34460089 Free PMC article. No abstract available.
Abstract
Introduction: We assessed the efficacy and safety of repository corticotropin injection (RCI; Acthar® Gel) for persistently active systemic lupus erythematosus (SLE) despite use of moderate-dose glucocorticoids.
Methods: This multicenter, double-blind, randomized, placebo-controlled study enrolled patients ≥ 18 years with active SLE and moderate to severe rash and/or arthritis despite stable glucocorticoid doses (7.5-30 mg/day prednisone equivalent) and antimalarials for ≥ 4 weeks and/or immunosuppressants for ≥ 8 weeks before screening. Stable glucocorticoid doses were required through week 16 with optional taper from weeks 16 to 24. Patients were randomized (1:1) to 80 U RCI subcutaneously or placebo every other day to week 4, then twice weekly to week 24. Endpoints included the proportion of SLE Responder Index (SRI)-4 responders at week 16; changes from baseline to week 16 in 28 Swollen Joint Count/Tender Joint Count (28 SJC/TJC) and Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI)-Activity score; and changes from baseline to week 24 in inflammatory cytokines. Safety was assessed by adverse events.
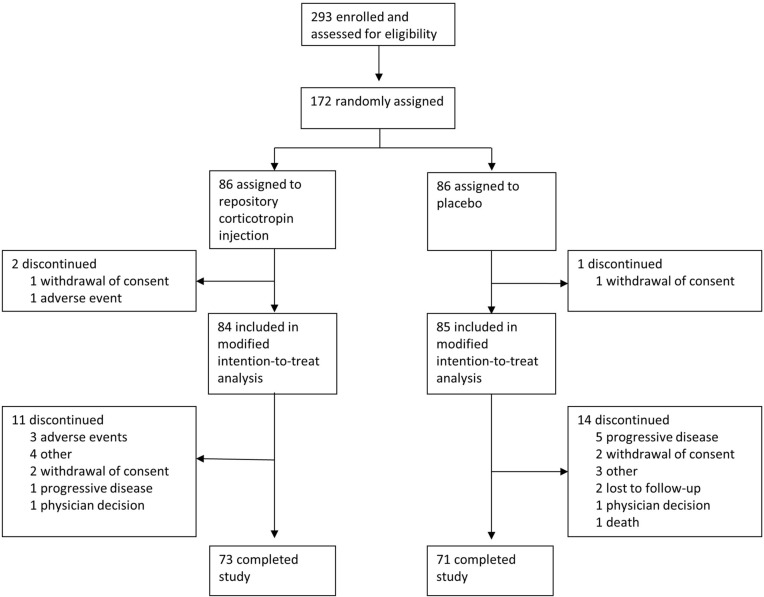
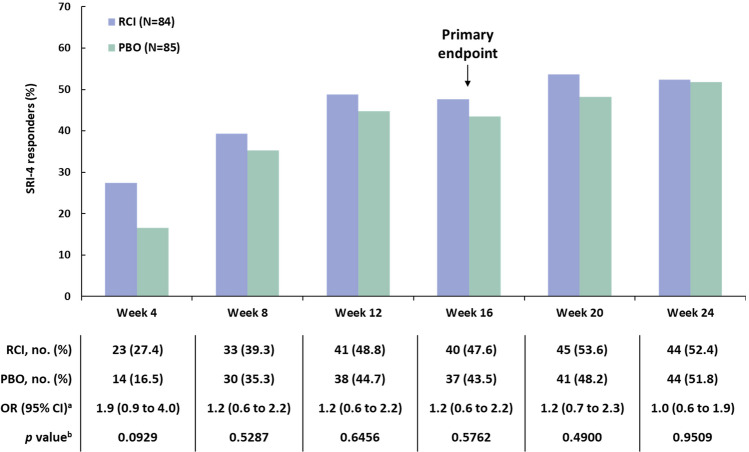
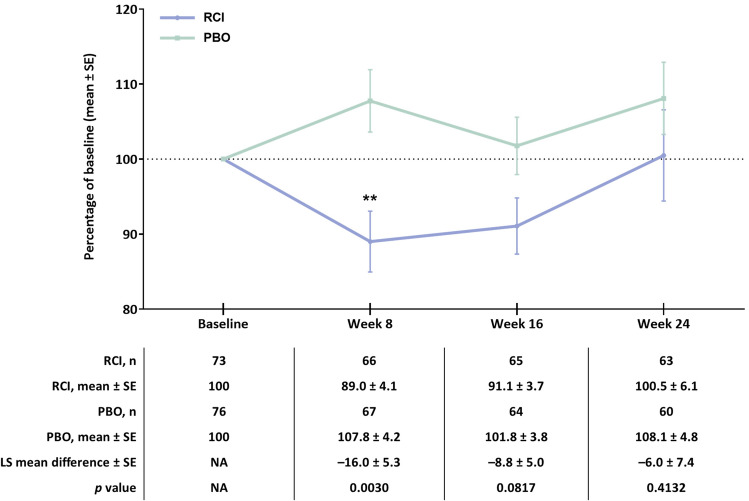
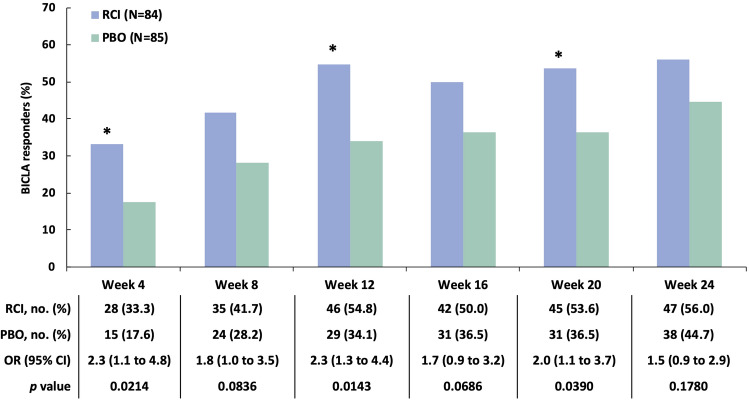
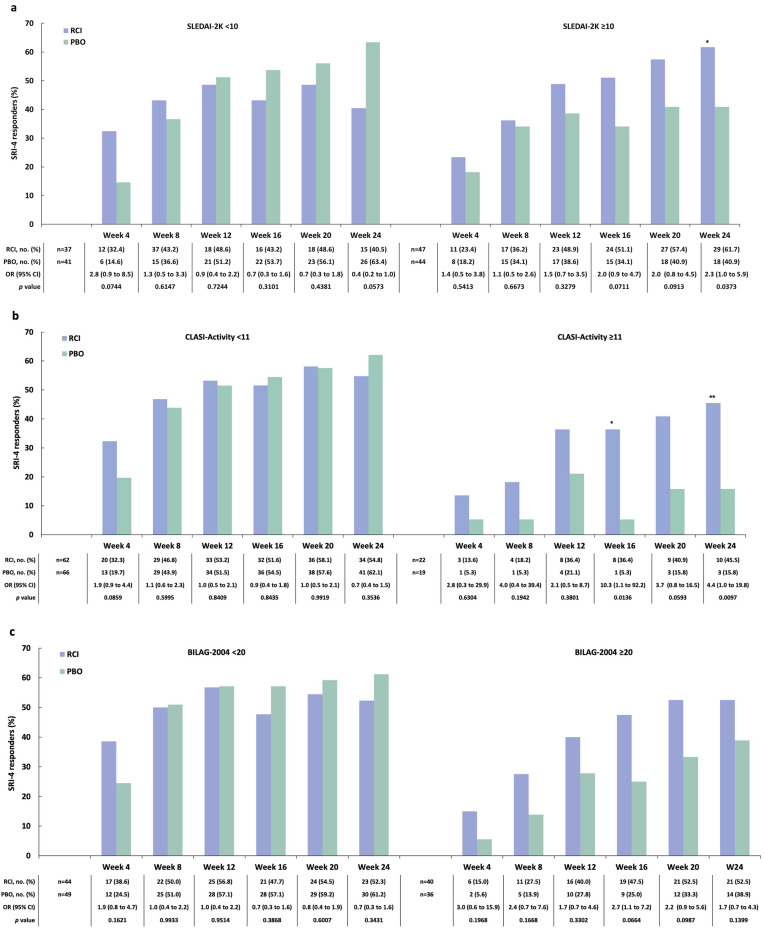
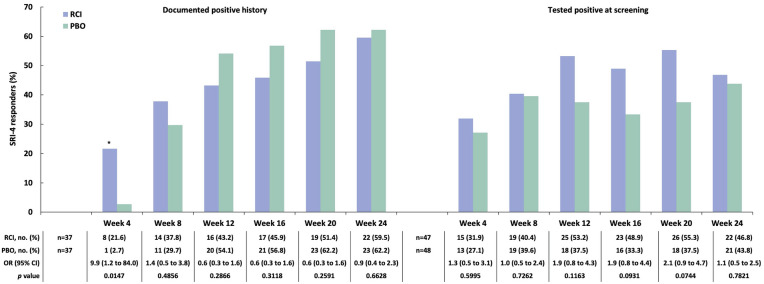
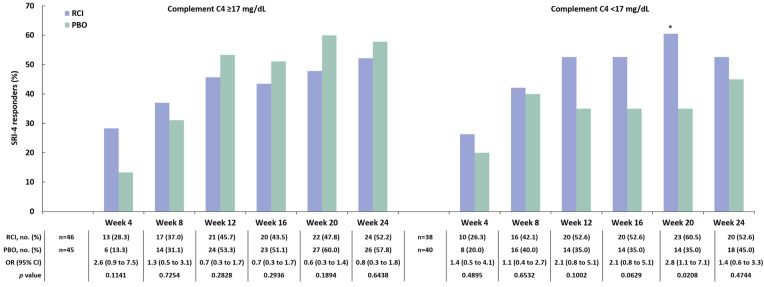
Results: In the modified intention-to-treat population (RCI, n = 84; placebo, n = 85), the proportion of SRI-4 responders at week 16 was not significantly different between groups (RCI, 47.6%; placebo, 43.5%; OR [95% CI] 1.2 [0.6 to 2.2]; p = 0.5762). RCI treatment resulted in a reduction from baseline to week 16 in 28 SJC/TJC and CLASI-Activity score and from baseline to week 8 in a proliferation-inducing ligand cytokine. Post hoc analyses demonstrated a greater proportion of BILAG-based Combined Lupus Assessment responders for RCI than placebo at weeks 4, 12, and 20 and greater SRI-4 response in RCI-treated patients with baseline SLE Disease Activity Index-2000 ≥ 10 and CLASI-Activity ≥ 11. No new safety signals were identified.
Conclusions: Despite failure to achieve the primary endpoint, these results support the utility of RCI for treating persistently active SLE.
Trial registration: ClinicalTrials.gov identifier NCT02953821.
Keywords: Acthar Gel; Autoimmune disease; Clinical trial; Corticosteroid; Glucocorticoid; Inflammation; Repository corticotropin injection; Systemic lupus erythematosus.
Figures
References
-
- Acthar Gel [package insert]. Bedminster, NJ: Mallinckrodt ARD LLC; 2019.
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
