

Anterior Pelvic Plane: A Potentially Useful Pelvic Anatomical Reference Plane in Assessing the Patients' Ideal Pelvic Parameters Without the Influence of Spinal Sagittal Deformity
- PMID: 32996359
- PMCID: PMC9109563
- DOI: 10.1177/2192568220958676
Anterior Pelvic Plane: A Potentially Useful Pelvic Anatomical Reference Plane in Assessing the Patients' Ideal Pelvic Parameters Without the Influence of Spinal Sagittal Deformity
Abstract
Study design: Observational study.
Objective: This study was aimed at investigating the reliability of anterior pelvic plane (APP) as an anatomical reference plane for assessing the patients' pelvic incidence in patients with ankylosing spondylitis kyphosis deformity.
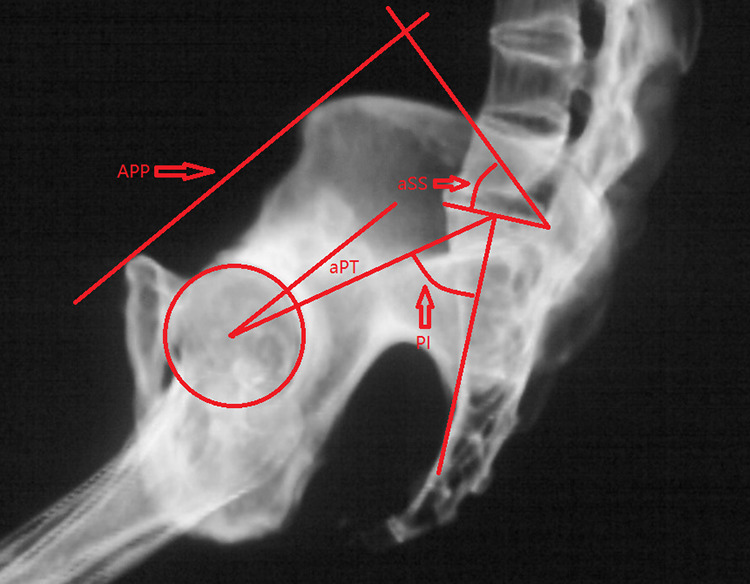
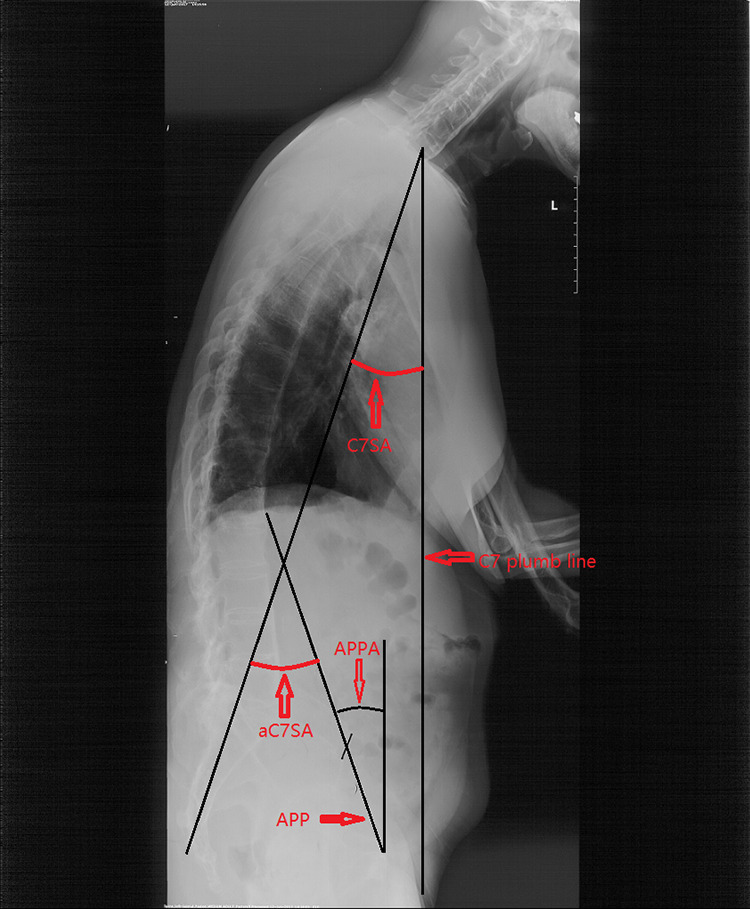
Methods: The globe kyphosis (GK), lumber lordosis (LL), thoracolumbar kyphosis (TLK), thoracic kyphosis (TK), anatomical cervical 7 sacrum angle (aC7SA), and cervical 7 sacrum angle (C7SA) were measured on full-length spine radiography imagines. The pelvic incidence (PI), anatomical pelvic tilt (aPT), and anatomical sacral slope (aSS) were measured on the pelvic synthesized 2D lateral radiography imagines. Because the angle between APP and vertical line was about 4°, Angle1 and tPT were calculated using the following formulas: Angle1 = aC7SA - 4; PT = aPT + 4. According to the study conducted by Vialle, traditional PT (tPT) was calculated using the following widely accepted formula: tPT = PI * 0.37 - 7. Measured PT (mPT) was also measured on the full-length spine radiography imagines.
Results: The data analysis showed that PI, mPT, aSS, aPT, and APPA were 50.83 ± 13.44°, 32.52 ± 4.64°, 41.36 ± 9.46°, 8.56 ± 6.80°, and 23.95 ± 5.17°, respectively. There was no significant difference between the PT and tPT (12.56 ± 6.80, 11.49 ± 4.73; P = .152). So, the results demonstrated that the PT could play the equivalent effect as tPT did for making surgical plans in patients with kyphosis deformity.
Conclusion: The pelvic anatomical reference plane had potential to be used in assessing the patients' ideal pelvic incident without the influence of spinal sagittal deformity. The aPT+4 may represent patients' postoperative ideal PT.
Keywords: anterior pelvic plane; pelvic incident.
Conflict of interest statement
Figures
Similar articles
-
Compensatory Mechanism of Maintaining the Sagittal Balance in Degenerative Lumbar Scoliosis Patients with Different Pelvic Incidence.Orthop Surg. 2020 Dec;12(6):1685-1692. doi: 10.1111/os.12805. Epub 2020 Sep 21. Orthop Surg. 2020. PMID: 32954650 Free PMC article.
-
Anatomical Pelvic Parameters Using the Anterior Pelvic Plane: Normative Values and Estimation of the Standing Sagittal Alignment in Healthy Volunteers.Spine Surg Relat Res. 2023 Nov 2;8(1):97-105. doi: 10.22603/ssrr.2023-0181. eCollection 2024 Jan 27. Spine Surg Relat Res. 2023. PMID: 38343408 Free PMC article.
-
Comparison of Sagittal Spinopelvic Alignment in Patients With Ankylosing Spondylitis and Thoracolumbar Fracture.Medicine (Baltimore). 2016 Jan;95(4):e2585. doi: 10.1097/MD.0000000000002585. Medicine (Baltimore). 2016. PMID: 26825904 Free PMC article.
-
Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults.Eur Spine J. 2013 Mar;22 Suppl 2(Suppl 2):S203-15. doi: 10.1007/s00586-012-2571-x. Epub 2012 Nov 28. Eur Spine J. 2013. PMID: 23188161 Free PMC article.
-
Increasing pelvic incidence is associated with more global sagittal imbalance in ankylosing spondylitis with thoracolumbar kyphosis: an observational retrospective study of 94 cases.BMC Musculoskelet Disord. 2020 Mar 27;21(1):192. doi: 10.1186/s12891-020-03226-0. BMC Musculoskelet Disord. 2020. PMID: 32220255 Free PMC article.
Cited by
-
Clinical Results of Utilizing the Satellite Rod Technique in Treating Ankylosing Spondylitis Kyphosis.Orthop Surg. 2022 Sep;14(9):2180-2187. doi: 10.1111/os.13427. Epub 2022 Aug 10. Orthop Surg. 2022. PMID: 35946438 Free PMC article.
-
The role of pelvic coronal parameters in determining sagittal balance: a prospective radiographic analysis of pelvic spinopelvic alignment in Chinese asymptomatic Han adolescents.Front Pediatr. 2025 Apr 14;13:1565338. doi: 10.3389/fped.2025.1565338. eCollection 2025. Front Pediatr. 2025. PMID: 40297555 Free PMC article.
-
A Comparison of Radiographic Outcomes after Total Hip Arthroplasty between the Direct Lateral Approach and Posterior Lateral Approach with EOS 2D/3D X-Ray Imaging System.Orthop Surg. 2023 May;15(5):1312-1324. doi: 10.1111/os.13726. Epub 2023 Apr 19. Orthop Surg. 2023. PMID: 37076774 Free PMC article.
-
Letter to the Editor Regarding "Normative Relationships Between Spinopelvic Alignment and Femoroacetabular Orientation: A Cross-Sectional Study".Global Spine J. 2025 Aug 7:21925682251367379. doi: 10.1177/21925682251367379. Online ahead of print. Global Spine J. 2025. PMID: 40773594 Free PMC article. No abstract available.
-
Impact of Flatback Deformity and Stiff Spinopelvic Mobility on 3-Dimensional Pelvic and Hip Kinematics After Total Hip Arthroplasty.JB JS Open Access. 2025 Mar 21;10(1):e24.00151. doi: 10.2106/JBJS.OA.24.00151. eCollection 2025 Jan-Mar. JB JS Open Access. 2025. PMID: 40124280 Free PMC article.
References
-
- Schwab F, Lafage V, Patel A, Farcy JP. Sagittal plane considerations and the pelvis in the adult patient. Spine (Phila Pa 1976). 2009;34:1828–1833. - PubMed
-
- Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010;35:2224–2231. - PubMed
-
- Noshchenko A, Ho, ffecker L, Cain CMJ, Patel VV, Burger EL. Spinopelvic parameters in asymptomatic subjects without spine disease and deformity: a systematic review with meta-analysis. Clin Spine Surg. 2017;30:392–403. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
