

Prior Anticoagulation in Patients with Ischemic Stroke and Atrial Fibrillation
- PMID: 32996627
- PMCID: PMC7756294
- DOI: 10.1002/ana.25917
Prior Anticoagulation in Patients with Ischemic Stroke and Atrial Fibrillation
Abstract
Objective: The aim was to evaluate, in patients with atrial fibrillation (AF) and acute ischemic stroke, the association of prior anticoagulation with vitamin K antagonists (VKAs) or direct oral anticoagulants (DOACs) with stroke severity, utilization of intravenous thrombolysis (IVT), safety of IVT, and 3-month outcomes.
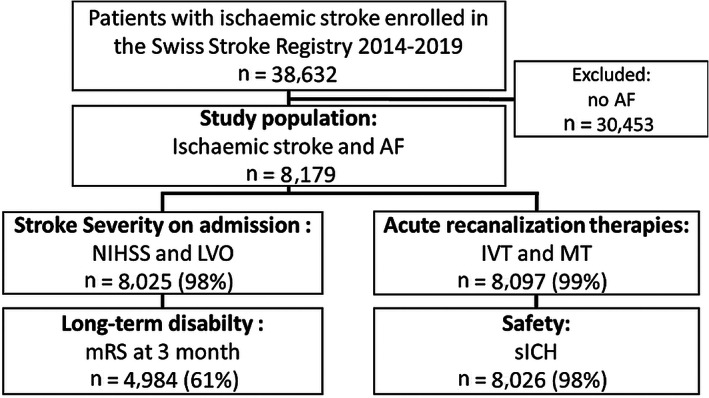
Methods: This was a cohort study of consecutive patients (2014-2019) on anticoagulation versus those without (controls) with regard to stroke severity, rates of IVT/mechanical thrombectomy, symptomatic intracranial hemorrhage (sICH), and favorable outcome (modified Rankin Scale score 0-2) at 3 months.
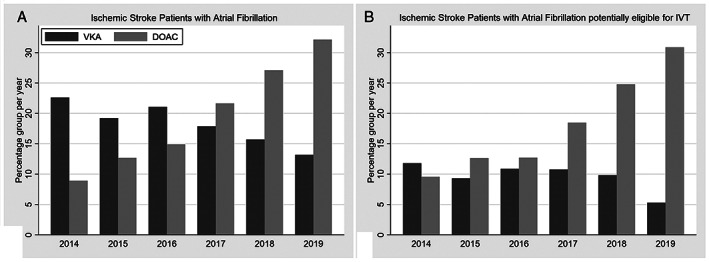
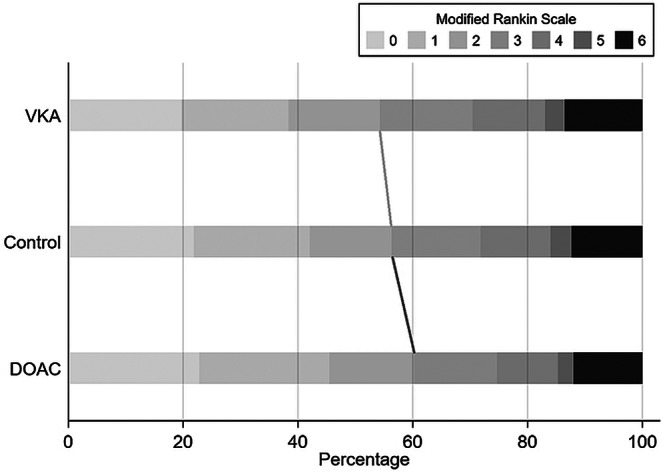
Results: Of 8,179 patients (mean [SD] age, 79.8 [9.6] years; 49% women), 1,486 (18%) were on VKA treatment, 1,634 (20%) on DOAC treatment at stroke onset, and 5,059 controls. Stroke severity was lower in patients on DOACs (median National Institutes of Health Stroke Scale 4, [interquartile range 2-11]) compared with VKA (6, [2-14]) and controls (7, [3-15], p < 0.001; quantile regression: β -2.1, 95% confidence interval [CI] -2.6 to -1.7). The IVT rate in potentially eligible patients was significantly lower in patients on VKA (156 of 247 [63%]; adjusted odds ratio [aOR] 0.67; 95% CI 0.50-0.90) and particularly in patients on DOACs (69 of 464 [15%]; aOR 0.06; 95% CI 0.05-0.08) compared with controls (1,544 of 2,504 [74%]). sICH after IVT occurred in 3.6% (2.6-4.7%) of controls, 9 of 195 (4.6%; 1.9-9.2%; aOR 0.93; 95% CI 0.46-1.90) patients on VKA and 2 of 65 (3.1%; 0.4-10.8%, aOR 0.56; 95% CI 0.28-1.12) of those on DOACs. After adjustments for prognostic confounders, DOAC pretreatment was associated with a favorable 3-month outcome (aOR 1.24; 1.01-1.51).
Interpretation: Prior DOAC therapy in patients with AF was associated with decreased admission stroke severity at onset and a remarkably low rate of IVT. Overall, patients on DOAC might have better functional outcome at 3 months. Further research is needed to overcome potential restrictions for IVT in patients taking DOACs. ANN NEUROL 2021;89:42-53.
© 2020 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The following companies manufacture drugs involved in this study: Bayer (BY; rivaroxaban), Boehringer Ingelheim (BI; dabigatran), Pfizer/Bristol Meyer Squibb (PB; apixaban), and Daiichi Sankyo (DS; edoxaban). M.A.: personal fees, BY, DS, and PB. P.Mic.: research grants, the ERISTA program (PB). M.R.H.: personal fees, BY. L.B.: consultancy or advisory board fees or speaker's honoraria and travel grants, BY and PB. M.K.: research funding, DS. C.B.: nonfinancial support, BI, PB, and BY. M.Bol.: nonfinancial support, BY. C.C.: personal fees, BY, BI, and PB. D.S.: other, PB. G.M.D.M.: personal fees, BY and PB. K.N.: personal fees, BY and PB. All other authors: nothing to report.
Figures
Comment in
-
Prior anticoagulation in patients with ischemic stroke and atrial fibrillation.Ann Neurol. 2021 Sep;90(3):517. doi: 10.1002/ana.26183. Epub 2021 Aug 10. Ann Neurol. 2021. PMID: 34331473 No abstract available.
-
Reply to "Prior Anticoagulation in Patients with Ischemic Stroke and Atrial Fibrillation".Ann Neurol. 2021 Sep;90(3):517-518. doi: 10.1002/ana.26184. Epub 2021 Aug 13. Ann Neurol. 2021. PMID: 34346522 No abstract available.
