

Evaluation of a National Comprehensive Cancer Network Guidelines-Based Decision Support Tool in Patients With Non-Small Cell Lung Cancer: A Nonrandomized Clinical Trial
- PMID: 32997124
- PMCID: PMC7527870
- DOI: 10.1001/jamanetworkopen.2020.9750
Evaluation of a National Comprehensive Cancer Network Guidelines-Based Decision Support Tool in Patients With Non-Small Cell Lung Cancer: A Nonrandomized Clinical Trial
Abstract
Importance: The association of guideline-based decision support with the quality of care in patients with non-small cell lung cancer (NSCLC) is not known.
Objective: To evaluate the association of exposure to the National Comprehensive Cancer Center (NCCN) guidelines with guideline-concordant care and patients' decisional conflict.
Design, setting, and participants: A nonrandomized clinical trial, conducted at a tertiary care academic institution, enrolled patients from February 23, 2015, to September 28, 2017. Data analysis was conducted from July 19, 2019, to April 22, 2020. A cohort of 76 patients with NSCLC seen at diagnosis or disease progression and a retrospective cohort of 157 patients treated before the trial were included. Adherence to 6 NCCN recommendations were evaluated: (1) smoking cessation counseling, (2) adjuvant chemotherapy for patients with stage IB to IIB NSCLC after surgery, (3) pathologic mediastinal staging in patients with stage III NSCLC before surgery, (4) pathologic mediastinal staging in patients with stage III NSCLC before nonsurgical treatment, (5) definitive chemoradiotherapy for patients with stage III NSCLC not having surgery, and (6) molecular testing for epidermal growth factor receptor and anaplastic lymphoma kinase alterations for patients with stage IV NSCLC. Subgroup analysis was conducted to compare the rates of guideline concordance between the prospective and retrospective cohorts. Secondary end points included decisional conflict and satisfaction.
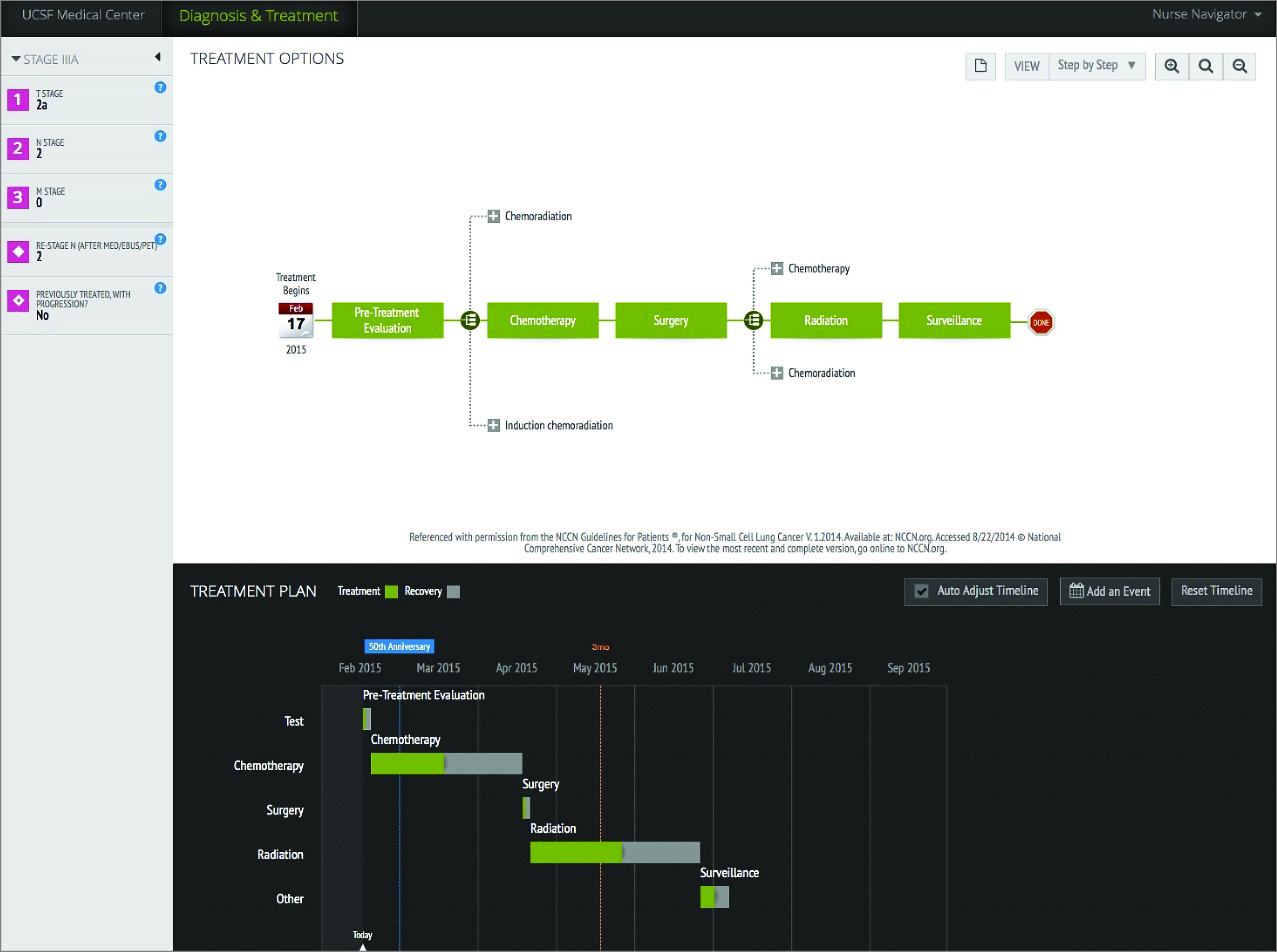
Interventions: An online tool customizing the NCCN guidelines to patients' clinical and pathologic features was used during consultation, facilitated by a trained coordinator.
Main outcomes and measures: Concordance of practice with 6 NCCN treatment recommendations on NSCLC and patients' decisional conflict.
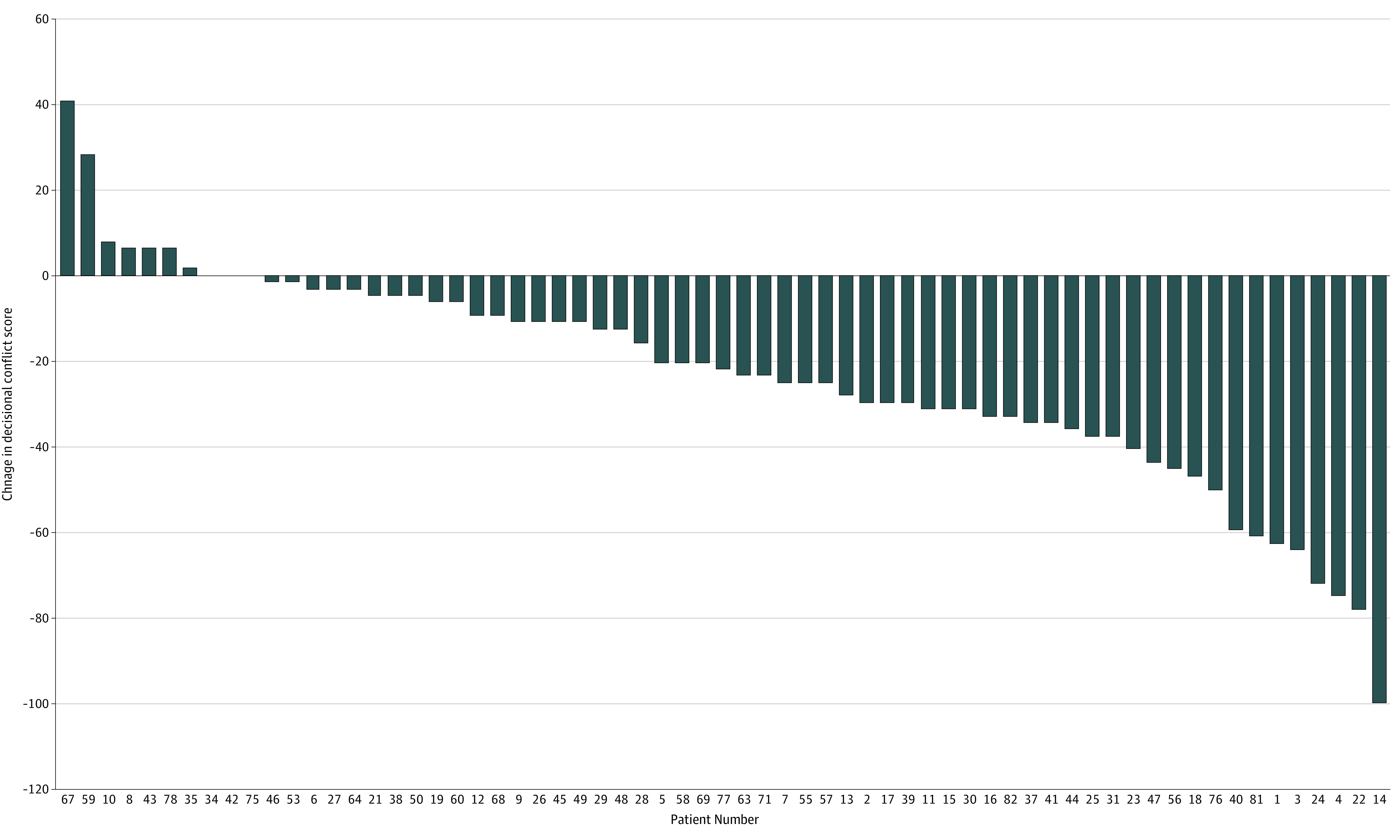
Results: Of the 76 patients with NSCLC, 44 were men (57.9%), median age at diagnosis was 68 years (interquartile range [IQR], 41-87 years), and 59 patients (77.6%) had adenocarcinoma. In the retrospective cohort, 91 of 157 patients (58.0%) were men, median age at diagnosis was 66 years (IQR, 61-65 years), and 105 patients (66.9%) had adenocarcinoma. After the intervention, patients received more smoking cessation counseling (4 of 5 [80.0%] vs 1 of 24 [4.2%], P < .001) and less adjuvant chemotherapy (0 of 7 vs 7 of 11 [63.6%]; P = .012). There was no significant change in mutation testing of non-squamous cell stage IV disease (20 of 20 [100%] vs 48 of 57 [84.2%]; P = .10). There was no significant change in pathologic mediastinal staging or initial chemoradiotherapy for patients with stage III disease. After consultation with the tool, decisional conflict scores improved by a median of 20 points (IQR, 3-34; P < .001).
Conclusions and relevance: The findings of this study suggest that exposure to the NCCN guidelines is associated with increased guideline-concordant care for 2 of 6 preselected recommendations and improvement in decisional conflict.
Trial registration: ClinicalTrials.gov Identifier: NCT03982459.
Conflict of interest statement
Figures
References
-
- Hacking B, Wallace L, Scott S, Kosmala-Anderson J, Belkora J, McNeill A. Testing the feasibility, acceptability and effectiveness of a ‘decision navigation’ intervention for early stage prostate cancer patients in Scotland–a randomised controlled trial. Psychooncology. 2013;22(5):1017-1024. doi: 10.1002/pon.3093 - DOI - PubMed
-
- Sun Q. Predicting Downstream Effects of High Decisional Conflict: Meta-analyses of the Decisional Conflict Scale. University of Ottawa; 2005.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
