

Association of Hypertension with All-Cause Mortality among Hospitalized Patients with COVID-19
- PMID: 32998337
- PMCID: PMC7650567
- DOI: 10.3390/jcm9103136
Association of Hypertension with All-Cause Mortality among Hospitalized Patients with COVID-19
Abstract
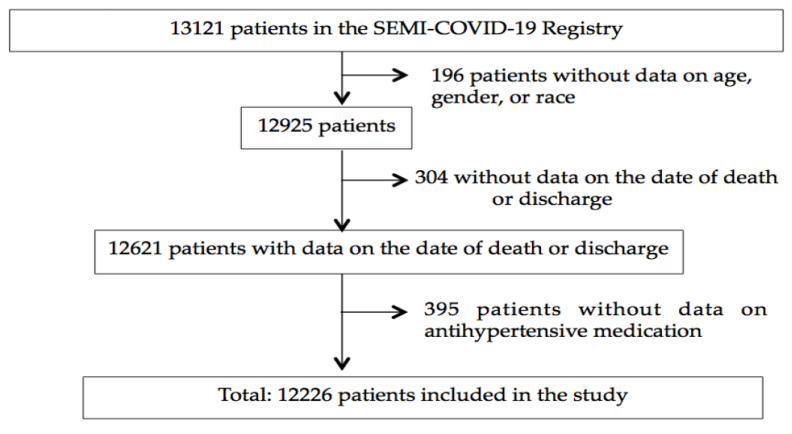
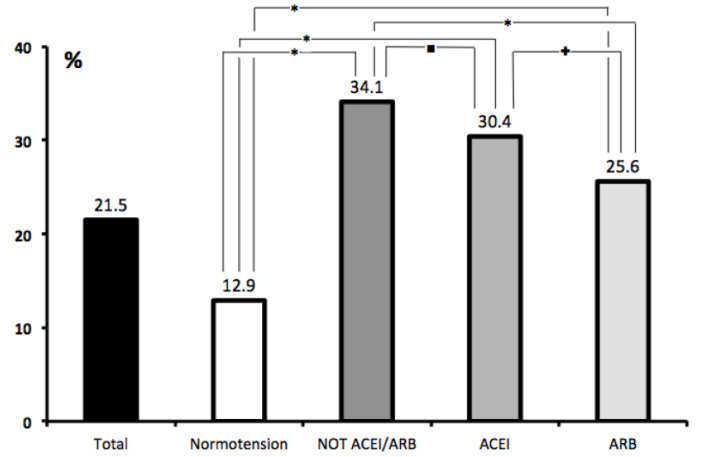
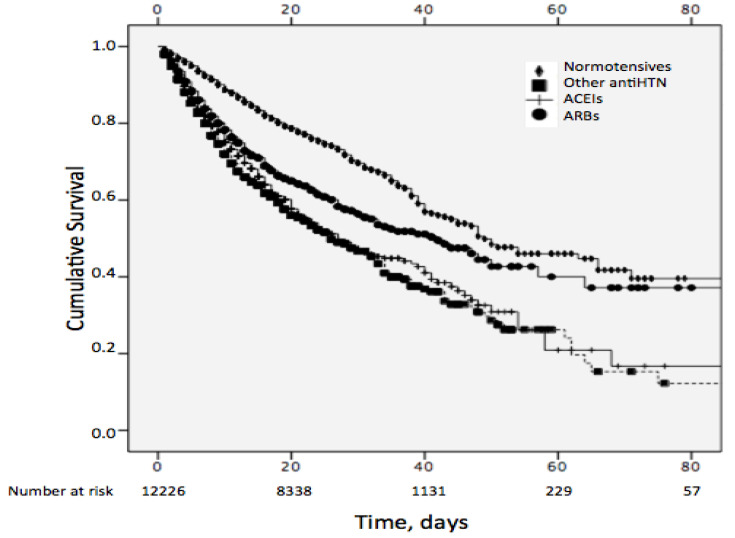
It is unclear to which extent the higher mortality associated with hypertension in the coronavirus disease (COVID-19) is due to its increased prevalence among older patients or to specific mechanisms. Cross-sectional, observational, retrospective multicenter study, analyzing 12226 patients who required hospital admission in 150 Spanish centers included in the nationwide SEMI-COVID-19 Network. We compared the clinical characteristics of survivors versus non-survivors. The mean age of the study population was 67.5 ± 16.1 years, 42.6% were women. Overall, 2630 (21.5%) subjects died. The most common comorbidity was hypertension (50.9%) followed by diabetes (19.1%), and atrial fibrillation (11.2%). Multivariate analysis showed that after adjusting for gender (males, OR: 1.5, p = 0.0001), age tertiles (second and third tertiles, OR: 2.0 and 4.7, p = 0.0001), and Charlson Comorbidity Index scores (second and third tertiles, OR: 4.7 and 8.1, p = 0.0001), hypertension was significantly predictive of all-cause mortality when this comorbidity was treated with angiotensin-converting enzyme inhibitors (ACEIs) (OR: 1.6, p = 0.002) or other than renin-angiotensin-aldosterone blockers (OR: 1.3, p = 0.001) or angiotensin II receptor blockers (ARBs) (OR: 1.2, p = 0.035). The preexisting condition of hypertension had an independent prognostic value for all-cause mortality in patients with COVID-19 who required hospitalization. ARBs showed a lower risk of lethality in hypertensive patients than other antihypertensive drugs.
Keywords: COVID-19; all-cause mortality; angiotensin II receptor blockers (ARBs); angiotensin-converting enzyme inhibitors (ACEIs); hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Johns Hopkins University Website. [(accessed on 14 August 2020)]; Available online: https://coronavirus.jhu.edu/map.html.
-
- Grasselli G., Zangrillo A., Zanella A., Massimo A., Luca C., Antonio C., Danilo C., Antonio C., Giuseppe F., Roberto F., et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region. JAMA. 2020;323:1574–1581. doi: 10.1001/jama.2020.5394. - DOI - PMC - PubMed
-
- Global Atlas on Cardiovascular Disease Prevention and Control. World Health Organization; Geneva, Switzerland: 2011.
-
- Liang W., Liang H., Ou L., Chen B., Chen A., Li C., Li Y., Guan W., Sang L., Lu J., et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Int. Med. 2020:e202033. doi: 10.1001/jamainternmed.2020.2033. - DOI - PMC - PubMed
