

Renin-Angiotensin System Blockers and Adverse Outcomes of Influenza and Pneumonia: A Danish Cohort Study
- PMID: 32998607
- PMCID: PMC7792378
- DOI: 10.1161/JAHA.120.017297
Renin-Angiotensin System Blockers and Adverse Outcomes of Influenza and Pneumonia: A Danish Cohort Study
Abstract
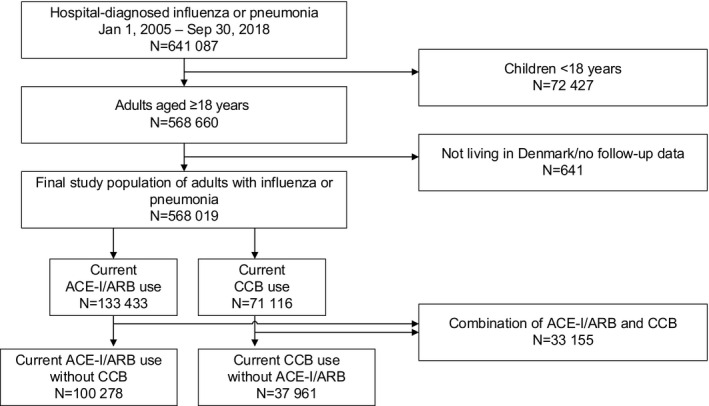
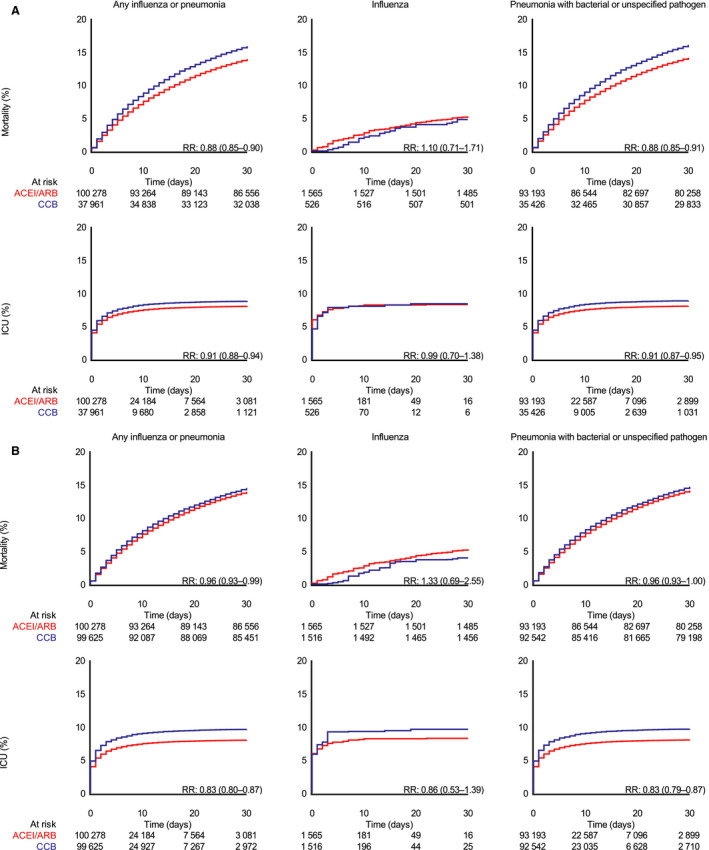
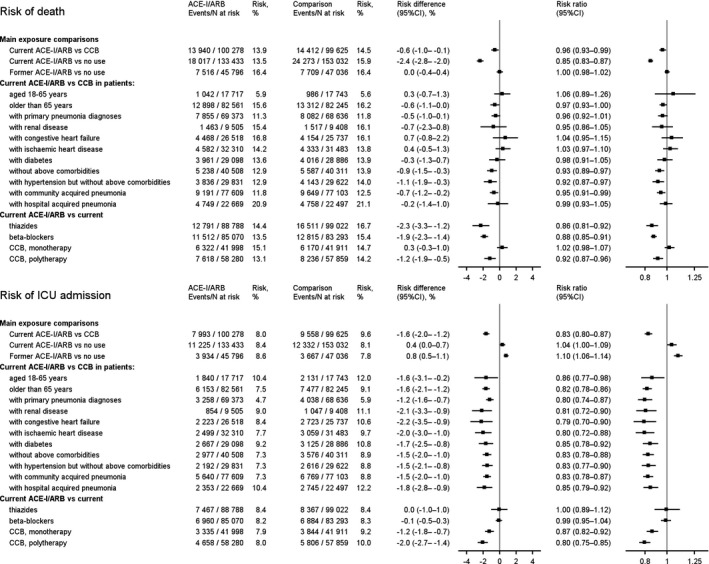
Background Angiotensin-converting enzyme inhibitors (ACE-Is) and angiotensin receptor blockers (ARBs) may worsen the prognosis of coronavirus disease 2019, but any association could be confounded by the cardiometabolic conditions indicating ACE-I/ARB use. We therefore examined the impact of ACE-Is/ARBs on respiratory tract infection outcomes. Methods and Results This cohort study included all adult patients hospitalized with influenza or pneumonia from 2005 to 2018 in Denmark using population-based medical databases. Thirty-day mortality and risk of admission to the intensive care unit in ACE-Is/ARBs users was compared with nonusers and with users of calcium channel blockers. We used propensity scores to handle confounding and computed propensity score-weighted risks, risk differences (RDs), and risk ratios (RRs). Of 568 019 patients hospitalized with influenza or pneumonia, 100 278 were ACE-I/ARB users and 37 961 were users of calcium channel blockers. In propensity score-weighted analyses, ACE-I/ARB users had marginally lower 30-day mortality than users of calcium channel blockers (13.9% versus 14.5%; RD, -0.6%; 95% CI, -1.0 to -0.1; RR, 0.96; 95% CI, 0.93-0.99), and a lower risk of admission to the intensive care unit (8.0% versus 9.6%; RD, -1.6%; 95% CI, -2.0 to -1.2; RR, 0.83; 95% CI, 0.80-0.87). Compared with nonusers, current ACE-I/ARB users had lower mortality (RD, -2.4%; 95% CI, -2.8 to -2.0; RR, 0.85; 95% CI, 0.83-0.87), but similar risk of admission to the intensive care unit (RD, 0.4%; 95% CI, 0.0-0.7; RR, 1.04; 95% CI, 1.00-1.09). Conclusions Among patients with influenza or pneumonia, ACE-I/ARB users had no increased risk of admission to the intensive care unit and slightly reduced mortality after controlling for confounding.
Keywords: angiotensin receptor blockers; angiotensin‐converting enzyme inhibitor; cohort study; infectious disease; intensive care unit.
Conflict of interest statement
Dr Christiansen, Dr Heide‐Jørgensen, Dr Rasmussen, Dr Thomsen, and Dr Sørensen have not received any personal fees, grants, travel grants, or teaching grants from companies, but the Department of Clinical Epidemiology is involved in studies with funding from various companies as research grants to (and administered by) Aarhus University. None of these studies are related to the current study. Dr Reilev, Dr Lund, Dr Pottegård, and Dr Hallas have participated in industry‐funded projects with money paid to their employer, University of Southern Denmark. None have received personal compensation of any kind, and none of these projects is related to the current study. The remaining authors have no disclosures to report.
Figures
References
-
- Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID‐19): a review. JAMA. 2020;1824–1836. - PubMed
-
- Sommerstein R, Gräni C. Rapid response: Re: preventing a covid‐19 pandemic: ACE inhibitors as a potential risk factor for fatal Covid‐19. BMJ. 2020;m810 Website name: . Available at: bmj.com https://www.bmj.com/content/368/bmj.M810/rr-2. Accessed August 14, 2020. - PubMed
-
- Patel AB, Verma A. COVID‐19 and angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers: what is the evidence? JAMA. 2020;1769–1770. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
