

Paenibacillus infection with frequent viral coinfection contributes to postinfectious hydrocephalus in Ugandan infants
- PMID: 32998967
- PMCID: PMC7774825
- DOI: 10.1126/scitranslmed.aba0565
Paenibacillus infection with frequent viral coinfection contributes to postinfectious hydrocephalus in Ugandan infants
Abstract
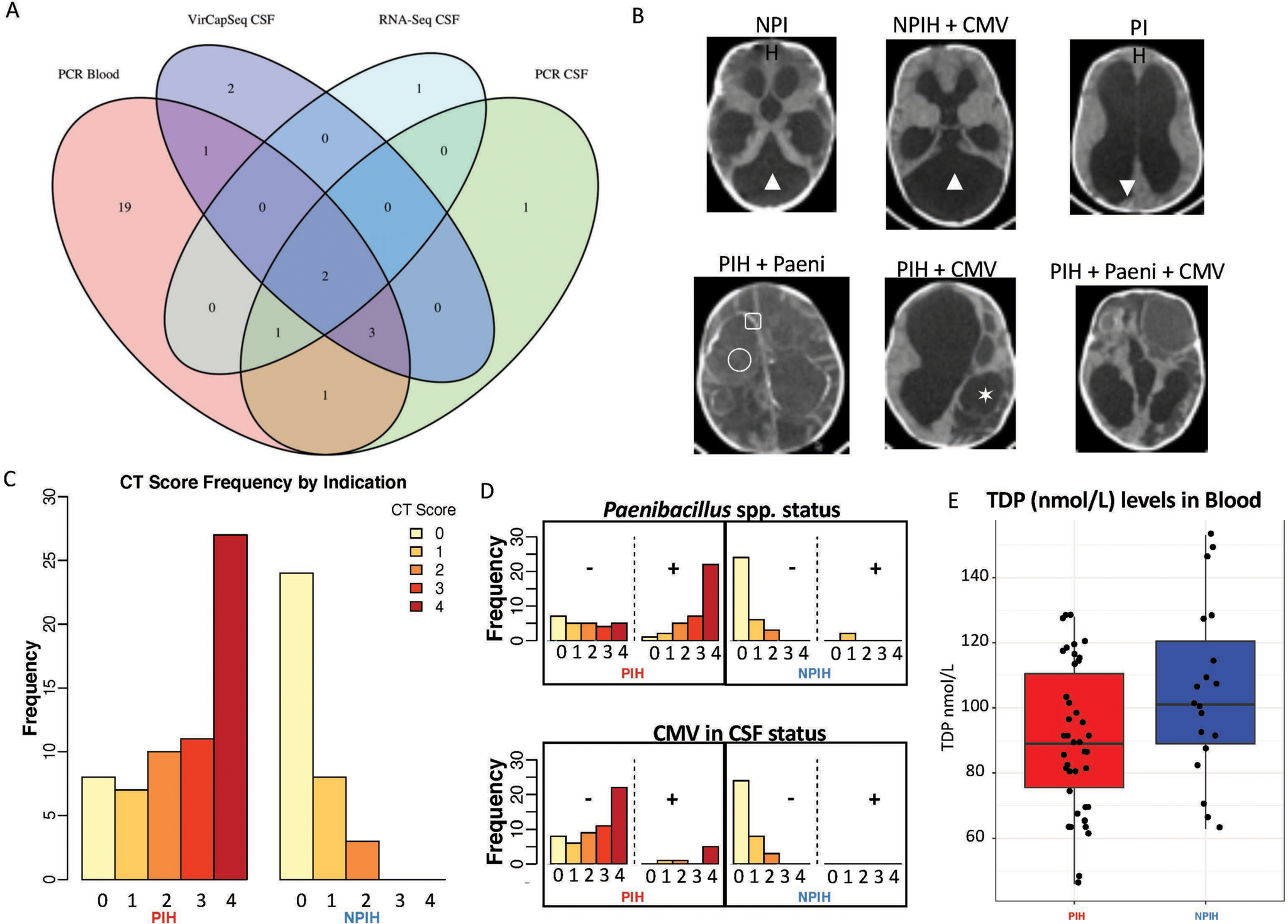
Postinfectious hydrocephalus (PIH), which often follows neonatal sepsis, is the most common cause of pediatric hydrocephalus worldwide, yet the microbial pathogens underlying this disease remain to be elucidated. Characterization of the microbial agents causing PIH would enable a shift from surgical palliation of cerebrospinal fluid (CSF) accumulation to prevention of the disease. Here, we examined blood and CSF samples collected from 100 consecutive infant cases of PIH and control cases comprising infants with non-postinfectious hydrocephalus in Uganda. Genomic sequencing of samples was undertaken to test for bacterial, fungal, and parasitic DNA; DNA and RNA sequencing was used to identify viruses; and bacterial culture recovery was used to identify potential causative organisms. We found that infection with the bacterium Paenibacillus, together with frequent cytomegalovirus (CMV) coinfection, was associated with PIH in our infant cohort. Assembly of the genome of a facultative anaerobic bacterial isolate recovered from cultures of CSF samples from PIH cases identified a strain of Paenibacillus thiaminolyticus This strain, designated Mbale, was lethal when injected into mice in contrast to the benign reference Paenibacillus strain. These findings show that an unbiased pan-microbial approach enabled characterization of Paenibacillus in CSF samples from PIH cases, and point toward a pathway of more optimal treatment and prevention for PIH and other proximate neonatal infections.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures





References
-
- Dewan MC, Rattani A, Mekary R, Glancz LJ, Yunusa I, Baticulon RE, Fieggen G, Wellons JC 3rd, Park KB, Warf BC, Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg, 1–15 (2018). - PubMed
-
- Warf BC, Hydrocephalus in Uganda: the predominance of infectious origin and primary management with endoscopic third ventriculostomy. Journal of neurosurgery 102, 1–15 (2005). - PubMed
-
- Warf BC, Alkire BC, Bhai S, Hughes C, Schiff SJ, Vincent JR, Meara JG, Costs and benefits of neurosurgical intervention for infant hydrocephalus in sub-Saharan Africa. Journal of neurosurgery Pediatrics 8, 509–521 (2011). - PubMed
-
- Aziz IA, Hydrocephalus in the Sudan. Journal of the Royal College of Surgeons of Edinburgh 21, 222–224 (1976). - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
