

Prevalence of Barrett's Epithelium Shown by Endoscopic Observations with Linked Color Imaging in Subjects with Different H. pylori Infection Statuses
- PMID: 32999237
- PMCID: PMC7990643
- DOI: 10.2169/internalmedicine.5676-20
Prevalence of Barrett's Epithelium Shown by Endoscopic Observations with Linked Color Imaging in Subjects with Different H. pylori Infection Statuses
Abstract
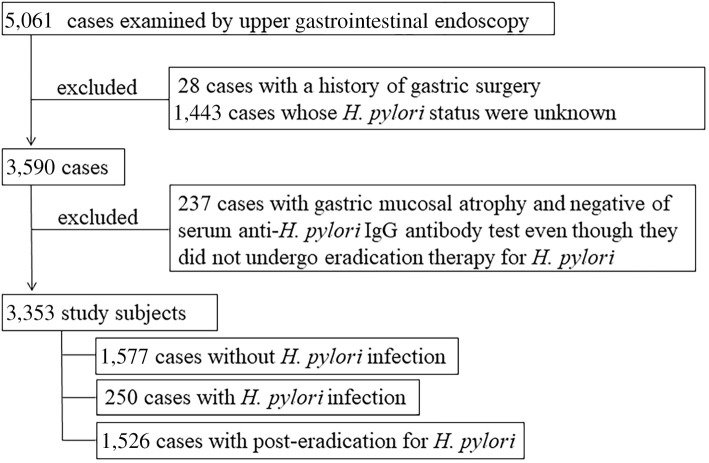
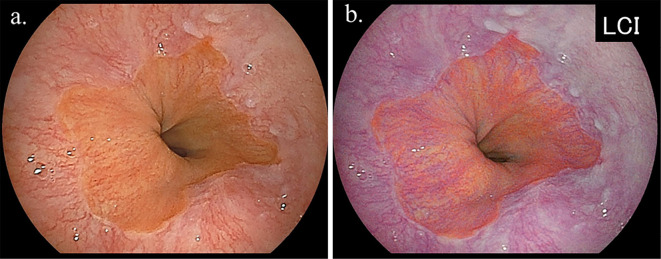
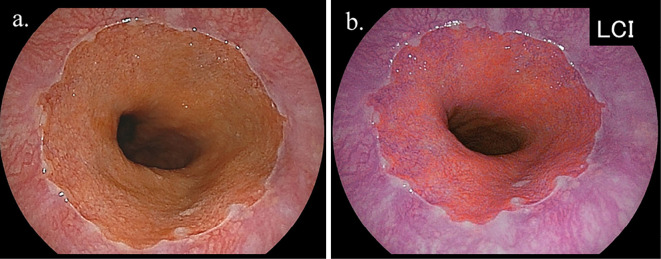
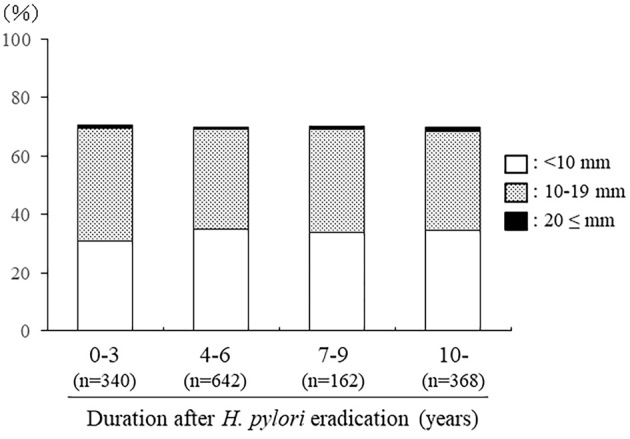
Objective This study was conducted to clarify the prevalence of short segment Barrett's esophagus (SSBE) using endoscopic observations with linked color imaging (LCI). In addition, the relationship between the presence of Barrett's epithelium (BE) and the status of H. pylori infection was investigated. Methods The study subjects were 3,353 individuals (2,186 men, 1,167 women; mean age 55.2±9.4 years old) whose status of H. pylori infection had been determined. An endoscopic observation using LCI was performed to examine the distal margin of palisade vessels and confirm the area of BE. The prevalence of BE ≥5 mm in length was investigated. Results BE was diagnosed in 1,884 (56.2%) subjects, with lengths of <10, 10-19, 20-29, and ≥30 mm found in 1,005, 851, 27, and 1, respectively. Its prevalence in H. pylori-negative, H. pylori-positive, and post-eradicated subjects was 41.7%, 64.4%, and 69.9%, respectively (p<0.001). The duration since successful eradication of H. pylori did not affect the prevalence of BE. The degree of gastric mucosal atrophy was higher in cases with BE (p<0.001), although negativity for H. pylori infection and mild gastric mucosal atrophy were significant factors for the development of longer BE. Conclusion A high prevalence of SSBE was noted when LCI was used to determine the area of BE, as the distal end of the palisade vessels was easily visualized. Negativity for H. pylori infection and mild gastric mucosal atrophy were not correlated with SSBE prevalence.
Keywords: Barrett's esophagus; Helicobacter pylori; LCI; SSBE; prevalence.
Conflict of interest statement
Figures
Similar articles
-
The prevalence of Helicobacter pylori infection and the status of gastric acid secretion in patients with Barrett's esophagus in Japan.Am J Gastroenterol. 2004 Jul;99(7):1213-21. doi: 10.1111/j.1572-0241.2004.30313.x. Am J Gastroenterol. 2004. PMID: 15233656
-
The impact of Helicobacter pylori on the presence of Barrett's esophagus in Azerbaijan, a high-prevalence area of infection.Dis Esophagus. 2019 Dec 30;32(11):doz053. doi: 10.1093/dote/doz053. Dis Esophagus. 2019. PMID: 31175364
-
Prevalence of Helicobacter pylori infection in 190 control subjects and in 236 patients with gastroesophageal reflux, erosive esophagitis or Barrett's esophagus.Dis Esophagus. 1997 Jan;10(1):38-42. doi: 10.1093/dote/10.1.38. Dis Esophagus. 1997. PMID: 9079272
-
Prevalence of Helicobacter pylori infection in 160 patients with Barrett's oesophagus or Barrett's adenocarcinoma.Aust N Z J Surg. 2000 Jan;70(1):26-33. doi: 10.1046/j.1440-1622.2000.01737.x. Aust N Z J Surg. 2000. PMID: 10696939 Review.
-
Helicobacter pylori and gastroesophageal reflux disease.Curr Opin Gastroenterol. 2014 Jul;30(4):402-7. doi: 10.1097/MOG.0000000000000085. Curr Opin Gastroenterol. 2014. PMID: 24848647 Review.
Cited by
-
Endoscopic diagnosis and screening of Barrett's esophagus: Inconsistency of diagnostic criteria between Japan and Western countries.DEN Open. 2021 Nov 15;2(1):e73. doi: 10.1002/deo2.73. eCollection 2022 Apr. DEN Open. 2021. PMID: 35310704 Free PMC article. Review.
-
Visibility Evaluation of Fundic Gland Polyp Associated With Proton Pump Inhibitor in Texture and Color Enhancement Imaging.DEN Open. 2025 May 22;6(1):e70147. doi: 10.1002/deo2.70147. eCollection 2026 Apr. DEN Open. 2025. PMID: 40406076 Free PMC article.
-
Kyoto international consensus report on anatomy, pathophysiology and clinical significance of the gastro-oesophageal junction.Gut. 2022 Aug;71(8):1488-1514. doi: 10.1136/gutjnl-2022-327281. Epub 2022 Jun 20. Gut. 2022. PMID: 35725291 Free PMC article.
-
Endoscopic findings of cardiac lymphoid hyperplasia and Helicobacter pylori infection status.DEN Open. 2021 Aug 22;2(1):e15. doi: 10.1002/deo2.15. eCollection 2022 Apr. DEN Open. 2021. PMID: 35310767 Free PMC article.
-
Development of an Artificial Intelligence Diagnostic System Using Linked Color Imaging for Barrett's Esophagus.J Clin Med. 2024 Mar 29;13(7):1990. doi: 10.3390/jcm13071990. J Clin Med. 2024. PMID: 38610762 Free PMC article.
References
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst 97: 142-146, 2005. - PubMed
-
- Everhart JE, Ruhl CE. Burden of digestive diseases in the United States part I: overall and upper gastrointestinal diseases. Gastroenterology 136: 376-386, 2009. - PubMed
-
- Hongo M, Nagasaki Y, Shoji T. Epidemiology of esophageal cancer: Orient to Occident. Effects of chronology, geography and ethnicity. J Gastroenterol Hepatol 24: 729-735, 2009. - PubMed
-
- Kusano C, Gotoda T, Khor CJ, et al. . Changing trends in the proportion of adenocarcinoma of the esophagogastric junction in a large tertiary referral center in Japan. J Gastroenterol Hepatol 23: 1662-1665, 2008. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical