

Magnetic resonance imaging of the shoulder
- PMID: 32999695
- PMCID: PMC7509696
- DOI: 10.5114/pjr.2020.98394
Magnetic resonance imaging of the shoulder
Abstract
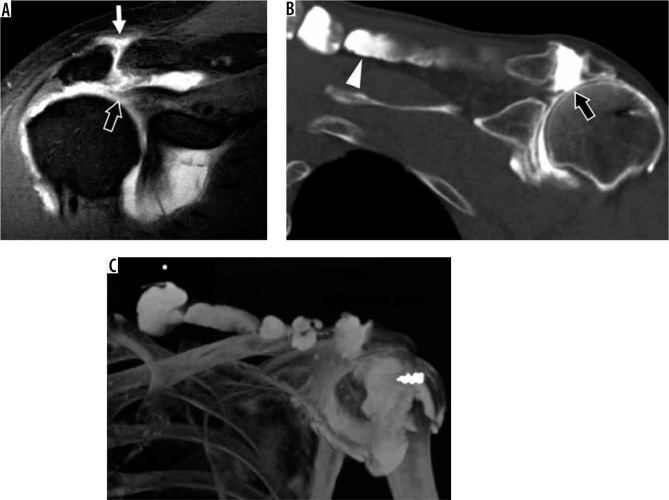
The aim of this article is to review the use of magnetic resonance imaging (MRI) for the evaluation of shoulder pain, which is a common clinical complaint of the musculoskeletal system. MRI is an essential auxiliary tool to evaluate these patients because of its high resolution and high sensitivity in depicting the soft tissues. This article will review the imaging technique, normal imaging anatomy, and most common imaging findings of disorders of tendons, labrum, and ligaments of the shoulder. It will also discuss common systemic diseases that manifest in the shoulder as well as disorders of the acromioclavicular joint and bursae. New advances and research in MRI have provided additional potential uses for evaluating shoulder derangements.
Keywords: MRI; acromioclavicular (AC) joint; glenohumeral joint; rotator cuff; shoulder.
Copyright © Polish Medical Society of Radiology 2020.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Luime JJ, Koes BW, Hendriksen IJ, et al. . Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand J Rheumatol 2004; 33: 73-81. - PubMed
-
- Davis SJ, Teresi LM, Bradley WG, et al. . Effect of arm rotation on MR imaging of the rotator cuff. Radiology 1991; 181: 265-268. - PubMed
-
- Chung CB., ea ACR–SPR–SSR Practice Parameter for the Performance and Interpretation of Magnetic Resonance Imaging (MRI) of the Shoulder. Available at: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/MR-Shldr.pdf?l... (Accessed: 03.02.2020).
-
- McMonagle JS VE. MRI of the shoulder: rotator cuff Published 2012. (Accessed: 06.02.2020).
Publication types
LinkOut - more resources
Full Text Sources