

Extracorporeal cardiopulmonary resuscitation for in- and out-of-hospital cardiac arrest: systematic review and meta-analysis of propensity score-matched cohort studies
- PMID: 33000057
- PMCID: PMC7493557
- DOI: 10.1002/emp2.12091
Extracorporeal cardiopulmonary resuscitation for in- and out-of-hospital cardiac arrest: systematic review and meta-analysis of propensity score-matched cohort studies
Abstract
Introduction: In this systematic review and meta-analysis of propensity score-matched cohort studies, we quantitatively summarize whether venoarterial extracorporeal membrane oxygenation (VA-ECMO) used as extracorporeal cardiopulmonary resuscitation (ECPR), compared with conventional cardiopulmonary resuscitation (CCPR), is associated with improved rates of 30-day and long-term favorable neurological outcomes and survival in patients resuscitated from in- and out-of-hospital cardiac arrest.
Methods: We searched MEDLINE via PubMed, Embase, Scopus, and Google Scholar for eligible studies on January 14, 2019. All searches were limited to studies published between January 2000 and January 2019. Two investigators independently evaluated the quality (or certainty) of evidence according to GRADE guidelines. Pooled results are presented as relative risks (RRs) with 95% confidence intervals (CIs).
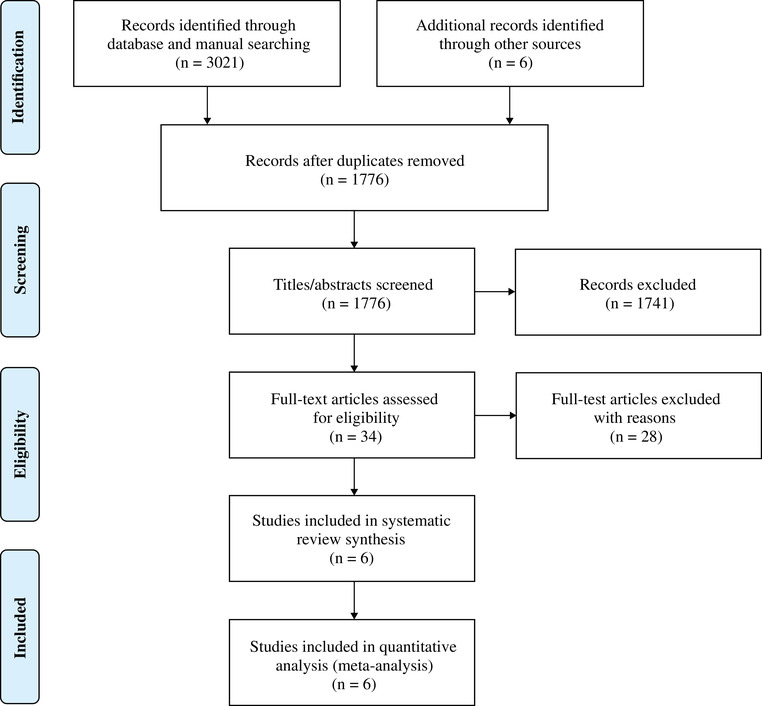
Results: Six cohort studies using propensity score-matched analysis were included, totaling 1108 matched patients. Pooled analyses showed that ECPR was likely associated with improved 30-day and long-term favorable neurological outcome in adults compared to CCPR for in- and out-of-hospital cardiac arrest (RR = 2.02, 95% CI = 1.29-3.16; I2 = 20%, P = 0.002; very low-quality evidence) and (RR = 2.86, 95% CI = 1.64-5.01; I2 = 0%, P = 0.0002; moderate-quality evidence), respectively. When we analyzed in- and out-of-hospital cardiac arrest separately, ECPR was likely associated with improved 30-day favorable neurological outcome compared to CCPR for in-hospital cardiac arrest (RR = 2.18, 95% CI = 1.24-3.81; I2 = 9%, P = 0.006; very low-quality evidence), but not for out-of-hospital cardiac arrest (RR = 2.61, 95% CI = 0.56-12.20; I2 = 59%, P = 0.22; very low-quality evidence). ECPR was also likely associated with improved long-term favorable neurological outcome compared to CCPR for in-hospital cardiac arrest (RR = 2.50, 95% CI = 1.33-4.71; I2 = 0%, P = 0.005; moderate-quality evidence) and out-of-hospital cardiac arrest (RR = 4.64, 95% CI = 1.41-15.25; I2 = 0%, P = 0.01; moderate-quality evidence).
Conclusions: Our analysis suggests that VA-ECMO used as ECPR may improve long-term favorable neurological outcomes and survival when compared to the best standard of care in a selected patient population. Therefore, it is imperative for well-designed randomized clinical trials to obtain a higher level of scientific evidence to ensure optimal outcomes for cardiac arrest patients.
Keywords: cardiopulmonary resuscitation; extracorporeal life support; extracorporeal membrane oxygenation; in‐hospital cardiac arrest; out‐of‐hospital cardiac arrest.
© 2020 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of the American College of Emergency Physicians.
Conflict of interest statement
None.
Figures




References
LinkOut - more resources
Full Text Sources