

Natural history of prostate cancer on active surveillance: stratification by MRI using the PRECISE recommendations in a UK cohort
- PMID: 33000302
- PMCID: PMC7880925
- DOI: 10.1007/s00330-020-07256-z
Natural history of prostate cancer on active surveillance: stratification by MRI using the PRECISE recommendations in a UK cohort
Abstract
Objectives: The PRECISE recommendations for magnetic resonance imaging (MRI) in patients on active surveillance (AS) for prostate cancer (PCa) include repeated measurement of each lesion, and attribution of a PRECISE radiological progression score for the likelihood of clinically significant change over time. We aimed to compare the PRECISE score with clinical progression in patients who are managed using an MRI-led AS protocol.
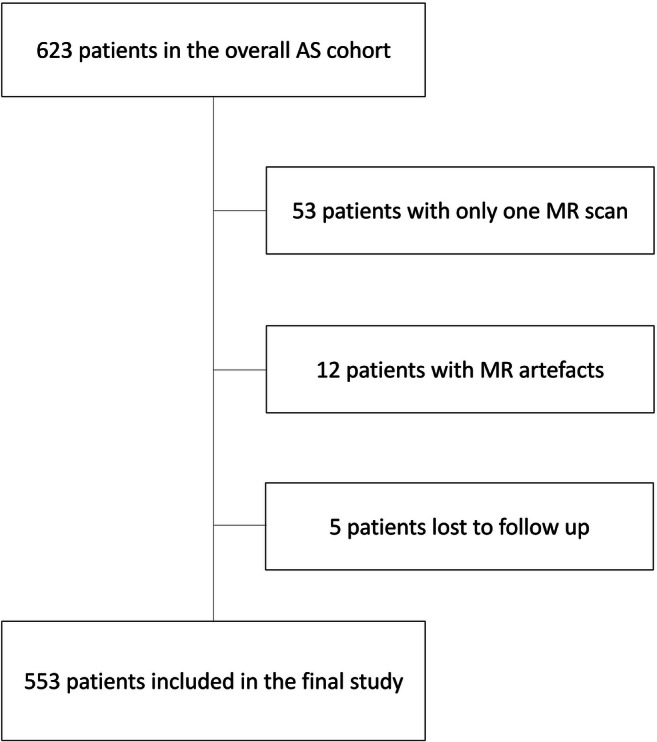
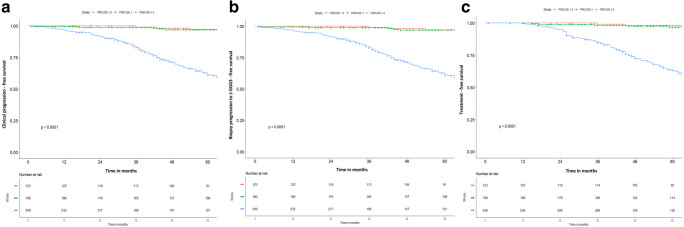
Methods: A total of 553 patients on AS for low- and intermediate-risk PCa (up to Gleason score 3 + 4) who had two or more MRI scans performed between December 2005 and January 2020 were included. Overall, 2161 scans were retrospectively re-reported by a dedicated radiologist to give a PI-RADS v2 score for each scan and assess the PRECISE score for each follow-up scan. Clinical progression was defined by histological progression to ≥ Gleason score 4 + 3 (Gleason Grade Group 3) and/or initiation of active treatment. Progression-free survival was assessed using Kaplan-Meier curves and log-rank test was used to assess differences between curves.
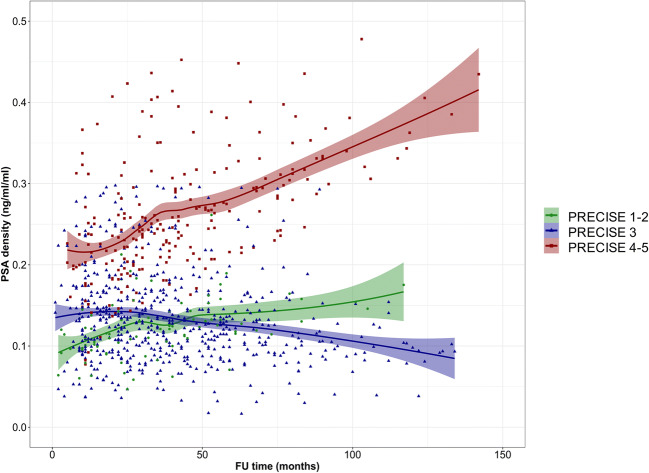
Results: Overall, 165/553 (30%) patients experienced the primary outcome of clinical progression (median follow-up, 74.5 months; interquartile ranges, 53-98). Of all patients, 313/553 (57%) did not show radiological progression on MRI (PRECISE 1-3), of which 296/313 (95%) had also no clinical progression. Of the remaining 240/553 patients (43%) with radiological progression on MRI (PRECISE 4-5), 146/240 (61%) experienced clinical progression (p < 0.0001). Patients with radiological progression on MRI (PRECISE 4-5) showed a trend to an increase in PSA density.
Conclusions: Patients without radiological progression on MRI (PRECISE 1-3) during AS had a very low likelihood of clinical progression and many could avoid routine re-biopsy.
Key points: • Patients without radiological progression on MRI (PRECISE 1-3) during AS had a very low likelihood of clinical progression and many could avoid routine re-biopsy. • Clinical progression was almost always detectable in patients with radiological progression on MRI (PRECISE 4-5) during AS. • Patients with radiological progression on MRI (PRECISE 4-5) during AS showed a trend to an increase in PSA density.
Keywords: Biopsy; Magnetic resonance imaging; Prostatic neoplasms; Urogenital neoplasms.
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
Francesco Giganti is funded by the UCL Graduate Research Scholarship and the Brahm PhD scholarship in memory of Chris Adams.
Vasilis Stavrinides is supported by an MRC Clinical Research Training Fellowship (MR/S005897/1) and has been previously supported by a UCL Bogue Fellowship and an EACR Travel Fellowship.
Bruce Trock has the following disclosures: Myriad Genetics, Inc.—research grant funding, advisory board; MDxHealth, Inc.—research grant funding; GenomeDX Biosciences, Inc.—consulting.
Shonit Punwani receives research support from the United Kingdom’s National Institute of Health Research (NIHR) UCLH/UCL Biomedical Research Centre.
Alex Kirkham is supported by the UCLH/UCL Biomedical Research Centre.
Mark Emberton is a United Kingdom National Institute of Health Research (NIHR) Senior Investigator and receives research support from the UCLH/UCL NIHR Biomedical Research Centre.
Caroline M Moore is supported by the UK NIHR, Movember, PCUK and the EAU Research Foundation.
Figures


Comment in
-
Editorial comment on "Natural history of prostate cancer on active surveillance: stratification by MRI using the PRECISE recommendations in a UK cohort".Eur Radiol. 2021 Mar;31(3):1642-1643. doi: 10.1007/s00330-020-07589-9. Epub 2021 Jan 8. Eur Radiol. 2021. PMID: 33416976 No abstract available.
References
-
- Schoots IG, Nieboer D, Giganti F, Moore CM, Bangma CH, Roobol MJ. Is magnetic resonance imaging-targeted biopsy a useful addition to systematic confirmatory biopsy in men on active surveillance for low-risk prostate cancer? A systematic review and meta-analysis. BJU Int. 2018;122(6):946–958. doi: 10.1111/bju.14358. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
