

Diagnostic accuracy of ultrasonography in the assessment of anterior knee pain
- PMID: 33000350
- PMCID: PMC7527384
- DOI: 10.1186/s13244-020-00914-2
Diagnostic accuracy of ultrasonography in the assessment of anterior knee pain
Abstract
Background: Anterior knee pain (AKP) is a problematic complaint, considered to be the most frequent cause of orthopedic consultancy for knee problems. This study aimed to highlight diagnostic accuracy of ultrasonography as a fast imaging technique in assessment of patients with AKP.
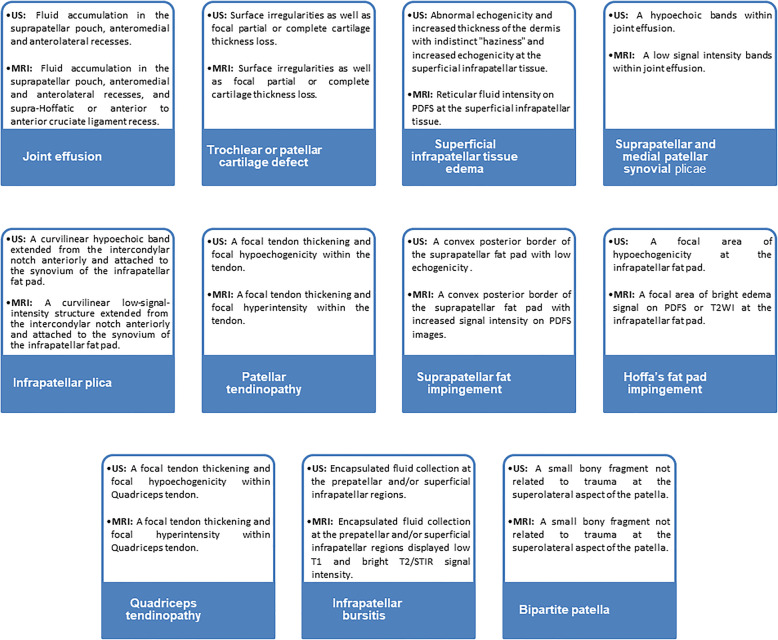
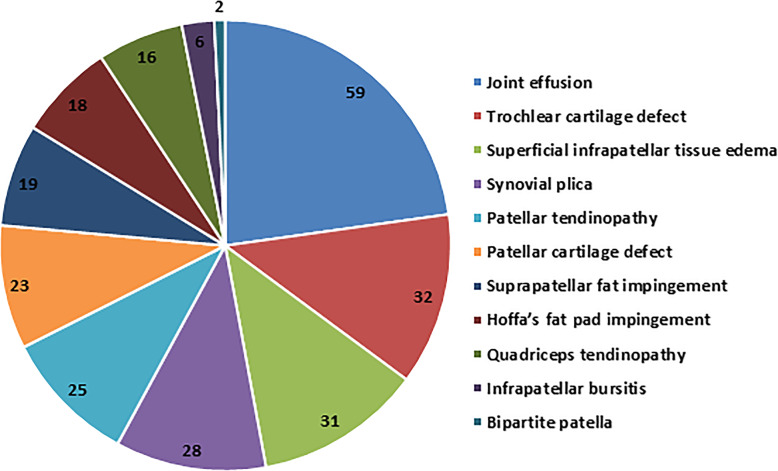
Methods and results: A prospective study was conducted on 143 patients with clinically confirmed AKP. All patients underwent ultrasonography and MRI examinations of the knee. The diagnostic accuracy of ultrasonography compared to MRI for evaluating different findings of possible causes of AKP were analyzed using receiver operating characteristic (ROC) curve and judged by area under curve (AUC). A total of 155 knees were included in the study; 26 knees showed no abnormalities, 19 knees showed positive MRI only, and 110 knees showed positive ultrasonography and MRI. Ultrasonography and MRI reported 11 different findings of possible causes of AKP or related to it. Joint effusion was the most common finding (38%) followed by trochlear cartilage defect (20.6%) and superficial infrapatellar subcutaneous edema (20%). The overall accuracy of ultrasonography was 85.3% sensitivity and 100% specificity. The ultrasonography provided the highest sensitivity (100%) in detecting bipartite patella, followed by 91.5% for joint effusion, and 87.5% for quadriceps tendinopathy. The ROC curve analysis of overall accuracy of ultrasonography showed an AUC of 0.93. The overall Kappa agreement between ultrasonography and MRI was good (k = 0.66).
Conclusion: Ultrasonography can be used to make a swift screening and assessment of painful anterior knee and as an alternative to MRI when it is unavailable or contraindicated.
Keywords: Anterior knee pain; Diagnostic accuracy; Knee joint; Magnetic resonance imaging; Ultrasonography.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
-
- Sanchis-alfonso V. Holistic approach to understanding anterior knee pain. Clinical implications. Knee Surg Sport Traumatol Arthrosc. 2014;22(10):2275–2285. - PubMed
-
- Whitlock K, Mosier B, Matzkin E (2018) Anterior Knee Pain: Diagnosis and Treatment. In: Katz J., Blauwet C., Schoenfeld A. (eds) Principles of Orthopedic Practice for Primary Care Providers. Springer, Cham. 19:313–327
-
- Samim M, Smitaman E, Lawrence D, Moukaddam H. MRI of anterior knee pain. Skeletal Radiol. 2014;43(7):875–893. - PubMed
-
- Hosny S, McClatchie W, Sofat N, Hing BC (2012) Knee pain in adults & adolescents, diagnosis and treatment. Pain Perspect. October. IntechOpen
LinkOut - more resources
Full Text Sources
