

18F-fluoride PET/MR in cardiac amyloid: A comparison study with aortic stenosis and age- and sex-matched controls
- PMID: 33000405
- PMCID: PMC8993737
- DOI: 10.1007/s12350-020-02356-1
18F-fluoride PET/MR in cardiac amyloid: A comparison study with aortic stenosis and age- and sex-matched controls
Abstract
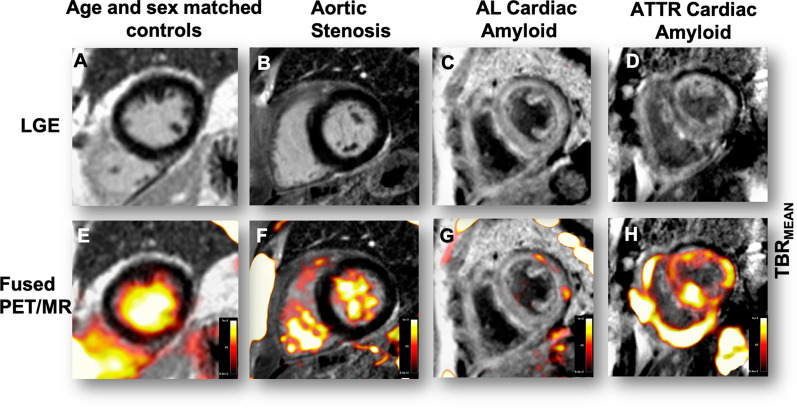
Objectives: Cardiac MR is widely used to diagnose cardiac amyloid, but cannot differentiate AL and ATTR subtypes: an important distinction given their differing treatments and prognoses. We used PET/MR imaging to quantify myocardial uptake of 18F-fluoride in ATTR and AL amyloid patients, as well as participants with aortic stenosis and age/sex-matched controls.
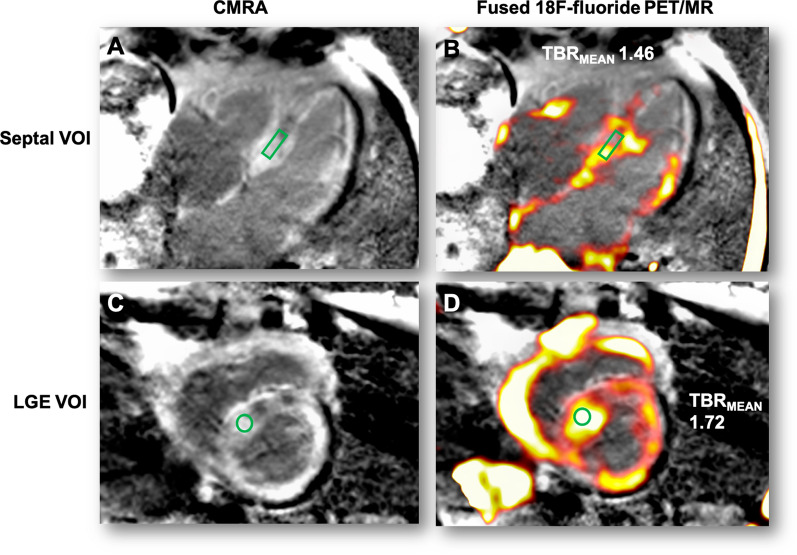
Methods: In this prospective multicenter study, patients were recruited in Edinburgh and New York and underwent 18F-fluoride PET/MR imaging. Standardized volumes of interest were drawn in the septum and areas of late gadolinium enhancement to derive myocardial standardized uptake values (SUV) and tissue-to-background ratio (TBRMEAN) after correction for blood pool activity in the right atrium.
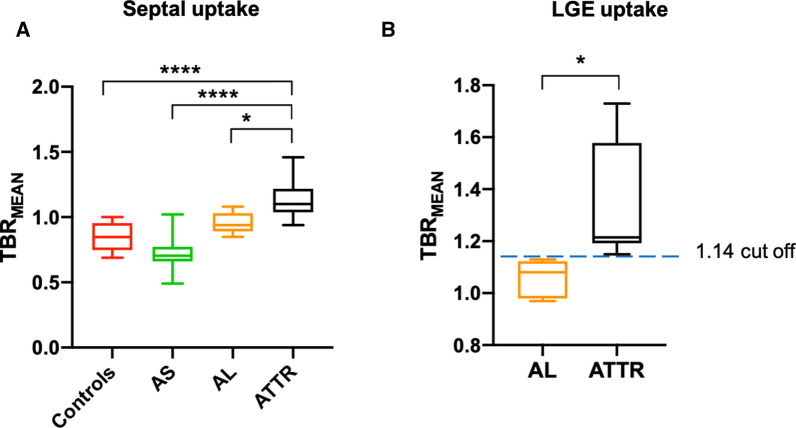
Results: 53 patients were scanned: 18 with cardiac amyloid (10 ATTR and 8 AL), 13 controls, and 22 with aortic stenosis. No differences in myocardial TBR values were observed between participants scanned in Edinburgh and New York. Mean myocardial TBRMEAN values in ATTR amyloid (1.13 ± 0.16) were higher than controls (0.84 ± 0.11, P = .0006), aortic stenosis (0.73 ± 0.12, P < .0001), and those with AL amyloid (0.96 ± 0.08, P = .01). TBRMEAN values within areas of late gadolinium enhancement provided discrimination between patients with ATTR (1.36 ± 0.23) and all other groups (e.g., AL [1.06 ± 0.07, P = .003]). A TBRMEAN threshold >1.14 in areas of LGE demonstrated 100% sensitivity (CI 72.25 to 100%) and 100% specificity (CI 67.56 to 100%) for ATTR compared to AL amyloid (AUC 1, P = .0004).
Conclusion: Quantitative 18F-fluoride PET/MR imaging can distinguish ATTR amyloid from other similar phenotypes and holds promise in improving the diagnosis of this condition.
Keywords: 18F-fluoride; Amyloid; Aortic stenosis; CMR; PET; PET/MR.
© 2020. The Author(s).
Figures
Comment in
-
Editorial: 18F-Fluoride PET/MR in cardiac amyloid; simple addition versus synergy?J Nucl Cardiol. 2022 Apr;29(2):750-752. doi: 10.1007/s12350-020-02437-1. Epub 2020 Nov 17. J Nucl Cardiol. 2022. PMID: 33205329 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- G0701127/MRC_/Medical Research Council/United Kingdom
- FS/17/79/33226/BHF_/British Heart Foundation/United Kingdom
- R01 HL071021/HL/NHLBI NIH HHS/United States
- FS/16/19/31982/BHF_/British Heart Foundation/United Kingdom
- T32 HL007824/HL/NHLBI NIH HHS/United States
- KL2 TR001435/TR/NCATS NIH HHS/United States
- FS/17/51/33096/BHF_/British Heart Foundation/United Kingdom
- FS/14/78/31020/BHF_/British Heart Foundation/United Kingdom
- RG/16/10/32375/BHF_/British Heart Foundation/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- FS/17/19/32641/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
