

Clinical Activity and Safety of the Anti-Programmed Death 1 Monoclonal Antibody Dostarlimab for Patients With Recurrent or Advanced Mismatch Repair-Deficient Endometrial Cancer: A Nonrandomized Phase 1 Clinical Trial
- PMID: 33001143
- PMCID: PMC7530821
- DOI: 10.1001/jamaoncol.2020.4515
Clinical Activity and Safety of the Anti-Programmed Death 1 Monoclonal Antibody Dostarlimab for Patients With Recurrent or Advanced Mismatch Repair-Deficient Endometrial Cancer: A Nonrandomized Phase 1 Clinical Trial
Abstract
Importance: Deficient mismatch mutation repair mechanisms may sensitize endometrial cancers to anti-programmed death 1 (PD-1) therapies. Dostarlimab (TSR-042) is an investigational anti-PD-1 antibody that binds with high affinity to the PD-1 receptor.
Objective: To assess the antitumor activity and safety of dostarlimab for patients with deficient mismatch repair endometrial cancer.
Design, setting, and participants: This ongoing, open-label, single-group, multicenter study began part 1 on March 7, 2016, and began enrolling patients with deficient mismatch mutation repair endometrial cancer on May 8, 2017. Median follow-up was 11.2 months (range, 0.03 [ongoing] to 22.11 [ongoing] months; based on radiological assessments). Statistical analysis was performed July 8 to August 9, 2019.
Interventions: Patients received 500 mg of dostarlimab intravenously every 3 weeks for 4 doses, then 1000 mg every 6 weeks until disease progression, treatment discontinuation, or withdrawal.
Main outcomes and measures: The primary end point was objective response rate and duration of response by blinded independent central review using Response Evaluation Criteria in Solid Tumors, version 1.1.
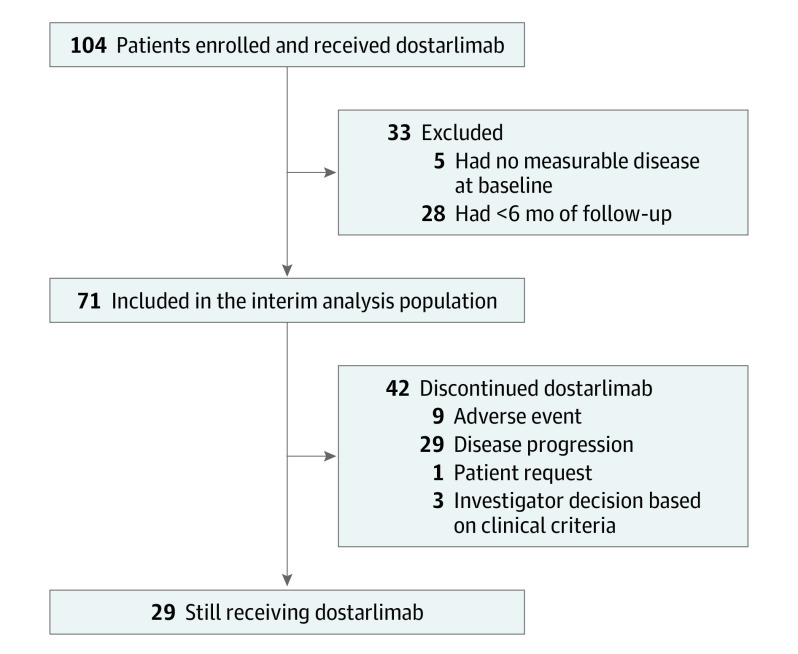
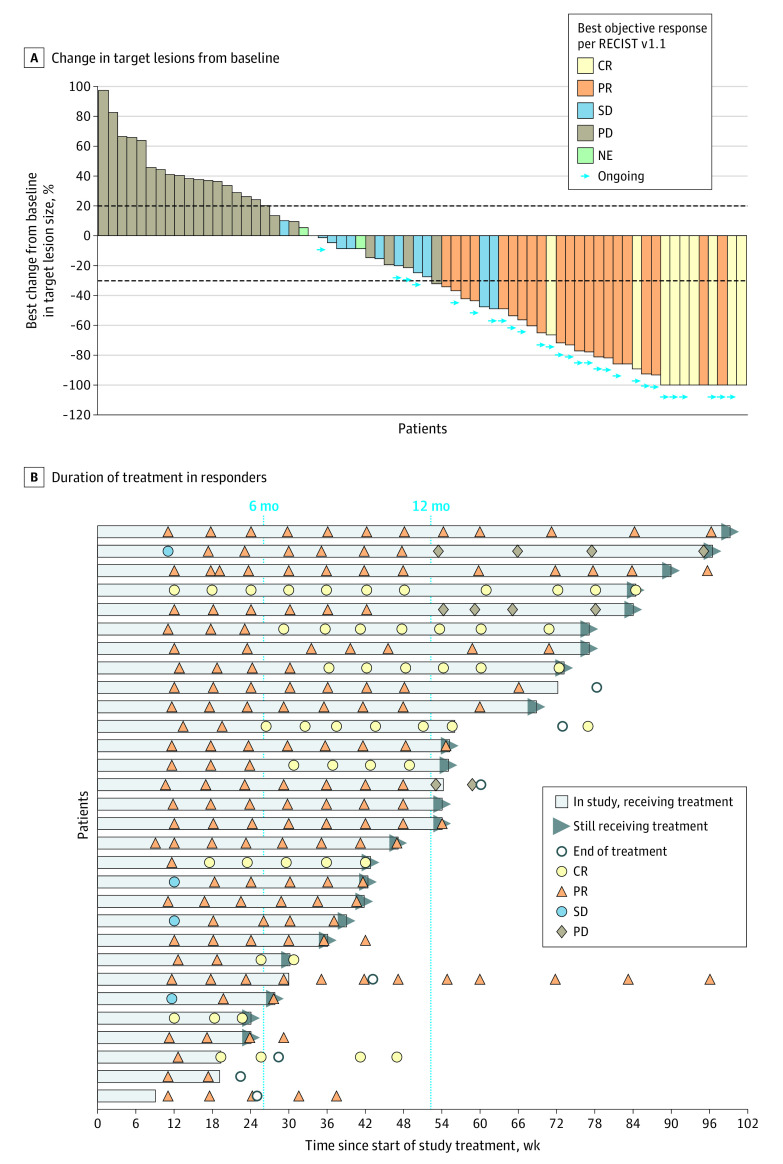
Results: As of the data cutoff, 104 women (median age, 64.0 years [range, 38-80 years]) with deficient mismatch mutation repair endometrial cancers were enrolled and treated with dostarlimab. Of these, 71 had measurable disease at baseline and at 6 months or more of follow-up and were included in the analysis. There was a confirmed response in 30 patients (objective response rate, 42.3%; 95% CI, 30.6%-54.6%); 9 patients (12.7%) had a confirmed complete response, and 21 patients (29.6%) had a confirmed partial response. Responses were durable; the median duration of response was not reached (median follow-up was 11.2 months). The estimated likelihood of maintaining a response was 96.4% at 6 months and 76.8% at 12 months. Anemia (3 of 104 [2.9%]), colitis (2 of 104 [1.9%]), and diarrhea (2 of 104 [1.9%]) were the most common grade 3 or higher treatment-related adverse events.
Conclusions and relevance: In this nonrandomized trial, dostarlimab was associated with clinically meaningful and durable antitumor activity with an acceptable safety profile for patients with deficient mismatch mutation repair endometrial cancers after prior platinum-based chemotherapy.
Trial registration: ClinicalTrials.gov identifier: NCT02715284.
Conflict of interest statement
Figures
Comment in
-
Clinical activity and safety of the anti-PD-1 monoclonal antibody dostarlimab for patients with recurrent or advanced dMMR endometrial cancer.Future Oncol. 2021 Oct 1;17(29):3781-3785. doi: 10.2217/fon-2021-0598. Epub 2021 Aug 24. Future Oncol. 2021. PMID: 34427115
References
-
- Garcia AA, Blessing JA, Nolte S, Mannel RS; Gynecologic Oncology Group . A phase II evaluation of weekly docetaxel in the treatment of recurrent or persistent endometrial carcinoma: a study by the Gynecologic Oncology Group. Gynecol Oncol. 2008;111(1):22-26. doi: 10.1016/j.ygyno.2008.06.013 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
