

LI-RADS category 5 hepatocellular carcinoma: preoperative gadoxetic acid-enhanced MRI for early recurrence risk stratification after curative resection
- PMID: 33001306
- PMCID: PMC7979599
- DOI: 10.1007/s00330-020-07303-9
LI-RADS category 5 hepatocellular carcinoma: preoperative gadoxetic acid-enhanced MRI for early recurrence risk stratification after curative resection
Abstract
Objectives: To explore the role of preoperative gadoxetic acid-enhanced MRI in stratifying the risk of early recurrence in patients with LR-5 hepatocellular carcinoma (HCC) by LI-RADS v2018 after curative resection.
Methods: Between July 2015 and August 2018, this study evaluated consecutive treatment-naïve at-risk LR-5 HCC patients who underwent gadoxetic acid-enhanced MRI examination within 2 weeks before curative resection. The Cox regression analysis was performed to identify potential predictors of early recurrence. Disease-free survival (DFS) rates were analyzed and compared by using the Kaplan-Meier method and log-rank tests.
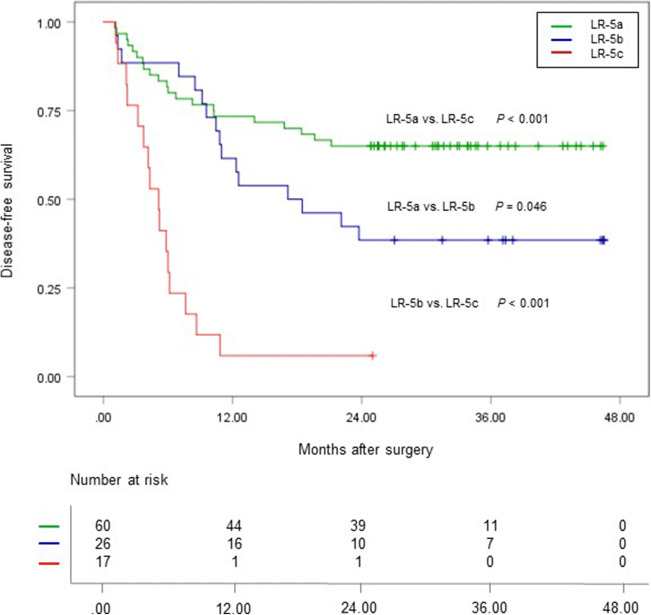
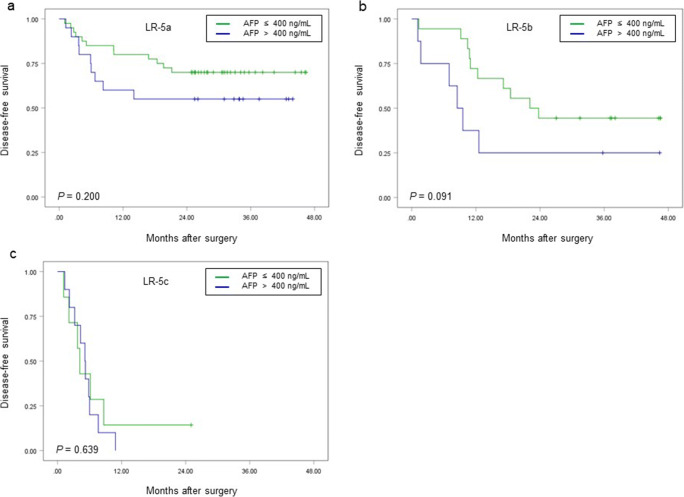
Results: Fifty-three of 103 (51.5%) patients experienced early recurrence. Three MRI findings were significantly associated with early recurrence: corona enhancement (hazard ratio [HR]: 2.116; p = 0.013), peritumoral hypointensity on hepatobiliary phase (HBP) (HR: 2.262; p = 0.007), and satellite nodule (HR: 2.777; p = 0.005). An additional risk factor was AFP level > 400 ng/mL (HR: 1.975; p = 0.016). Based on the number of MRI predictors, LR-5 HCC patients were stratified into three subgroups: LR-5a (60/103; no predictor), LR-5b (26/103; one predictor), and LR-5c (17/103; two or three predictors), with low, medium, and high risk of early recurrence, respectively. The 2-year DFS rate of LR-5a, LR-5b, and LR-5c patients was 65.0%, 38.5%, and 5.9%, respectively, while the corresponding median DFS was undefined, 17.1 months, and 5.1 months, respectively (p < 0.001).
Conclusions: In at-risk LR-5 HCC patients, corona enhancement, peritumoral hypointensity on HBP, and satellite nodule could be used to preoperatively stratify the risk of early recurrence after hepatectomy.
Key points: • Corona enhancement, peritumoral hypointensity on HBP, satellite nodule, and serum AFP level > 400 ng/mL were significant predictors of early recurrence in patients with LR-5 HCC after hepatectomy. • Based on the number of predictive MRI findings, LR-5 HCC patients could be preoperatively stratified into three subgroups: LR-5a, LR-5b, and LR-5c, with significantly different risk of early recurrence and disease-free survival. • Preoperative risk stratification is essential for the identification of patients at increased risk of postoperative early recurrence, which may contribute to risk-based personalized management for LR-5 HCC patients.
Keywords: Carcinoma, hepatocellular; Gadoxetic acid; Liver; Magnetic resonance imaging; Prognosis.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
Hepatocellular carcinoma: preoperative gadoxetic acid-enhanced MR imaging can predict early recurrence after curative resection using image features and texture analysis.Abdom Radiol (NY). 2019 Feb;44(2):539-548. doi: 10.1007/s00261-018-1768-9. Abdom Radiol (NY). 2019. PMID: 30229421
-
Gadoxetic acid-enhanced MRI as a predictor of recurrence of HCC after liver transplantation.Eur Radiol. 2020 Feb;30(2):987-995. doi: 10.1007/s00330-019-06424-0. Epub 2019 Aug 30. Eur Radiol. 2020. PMID: 31471754
-
Effect of combining serum alpha-fetoprotein with LI-RADS v2018 on gadoxetate-enhanced MRI in the diagnosis and prognostication of hepatocellular carcinoma.Eur Radiol. 2025 Aug;35(8):4957-4966. doi: 10.1007/s00330-025-11418-2. Epub 2025 Feb 10. Eur Radiol. 2025. PMID: 39930127
-
Hepatobiliary phase hypointense nodule without arterial phase hyperenhancement: are they at risk of HCC recurrence after ablation or surgery? A systematic review and meta-analysis.Eur Radiol. 2020 Mar;30(3):1624-1633. doi: 10.1007/s00330-019-06499-9. Epub 2019 Nov 27. Eur Radiol. 2020. PMID: 31776747
-
MRI imaging features for predicting macrotrabecular-massive subtype hepatocellular carcinoma: a systematic review and meta-analysis.Eur Radiol. 2024 Oct;34(10):6896-6907. doi: 10.1007/s00330-024-10671-1. Epub 2024 Mar 20. Eur Radiol. 2024. PMID: 38507054
Cited by
-
Estimating postsurgical outcomes of patients with a single hepatocellular carcinoma using gadoxetic acid-enhanced MRI: risk scoring system development and validation.Eur Radiol. 2023 May;33(5):3566-3579. doi: 10.1007/s00330-023-09539-7. Epub 2023 Mar 18. Eur Radiol. 2023. PMID: 36933020
-
Prognostic and predictive imaging markers of hepatocellular carcinoma: a pictorial essay.Insights Imaging. 2025 Aug 15;16(1):181. doi: 10.1186/s13244-025-02058-7. Insights Imaging. 2025. PMID: 40815430 Free PMC article.
-
Identification of vessels encapsulating tumor clusters in solitary hepatocellular carcinoma via imaging biomarkers in preoperative contrast-enhanced magnetic resonance imaging.Quant Imaging Med Surg. 2024 Dec 5;14(12):8586-8600. doi: 10.21037/qims-24-315. Epub 2024 Oct 17. Quant Imaging Med Surg. 2024. PMID: 39698687 Free PMC article.
-
Preoperative Prediction of a Rare and Highly Aggressive Subtype of Hepatocellular Carcinoma Based on Multimodal Imaging and Clinical Indicators.J Hepatocell Carcinoma. 2025 Jun 30;12:1253-1266. doi: 10.2147/JHC.S533963. eCollection 2025. J Hepatocell Carcinoma. 2025. PMID: 40620669 Free PMC article.
-
Up-to-Date Role of CT/MRI LI-RADS in Hepatocellular Carcinoma.J Hepatocell Carcinoma. 2021 May 31;8:513-527. doi: 10.2147/JHC.S268288. eCollection 2021. J Hepatocell Carcinoma. 2021. PMID: 34104640 Free PMC article. Review.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
