

Sarcopenia during COVID-19 lockdown restrictions: long-term health effects of short-term muscle loss
- PMID: 33001410
- PMCID: PMC7528158
- DOI: 10.1007/s11357-020-00272-3
Sarcopenia during COVID-19 lockdown restrictions: long-term health effects of short-term muscle loss
Abstract
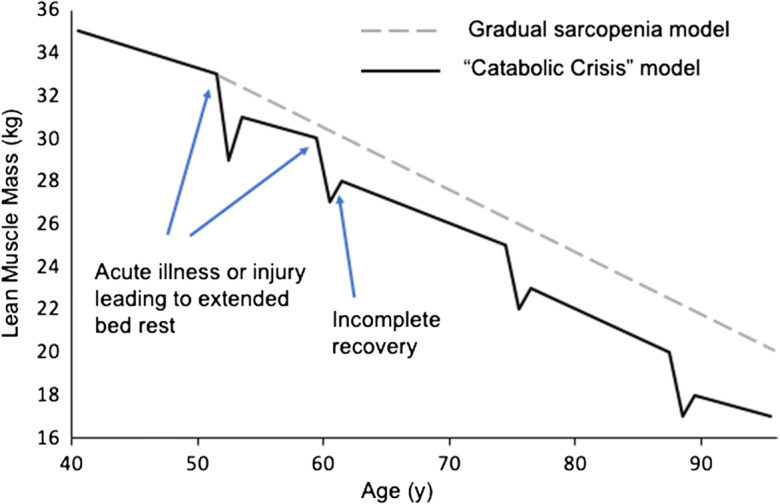
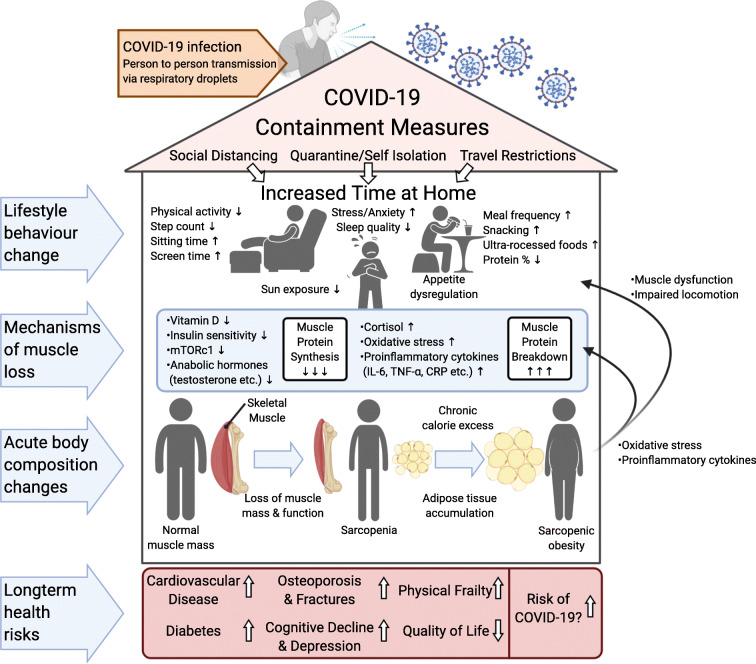
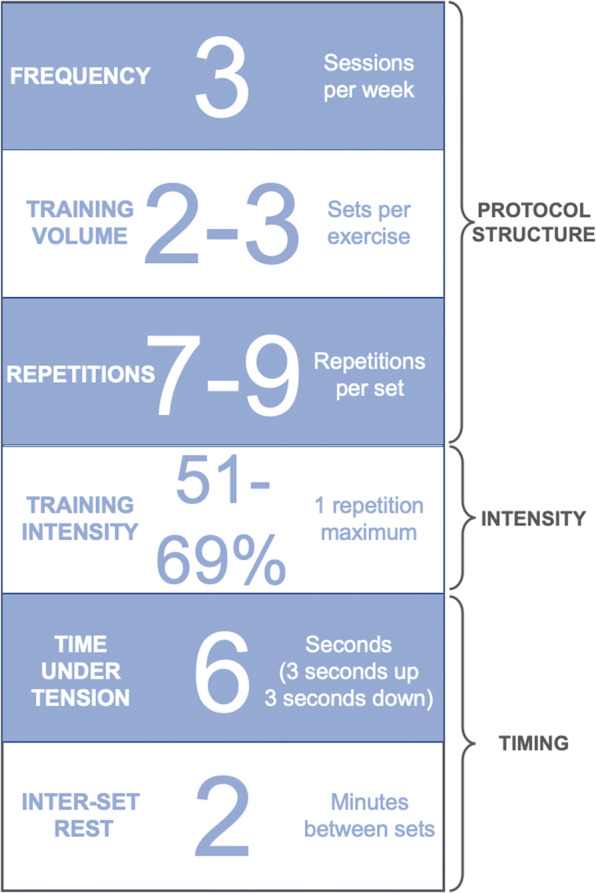
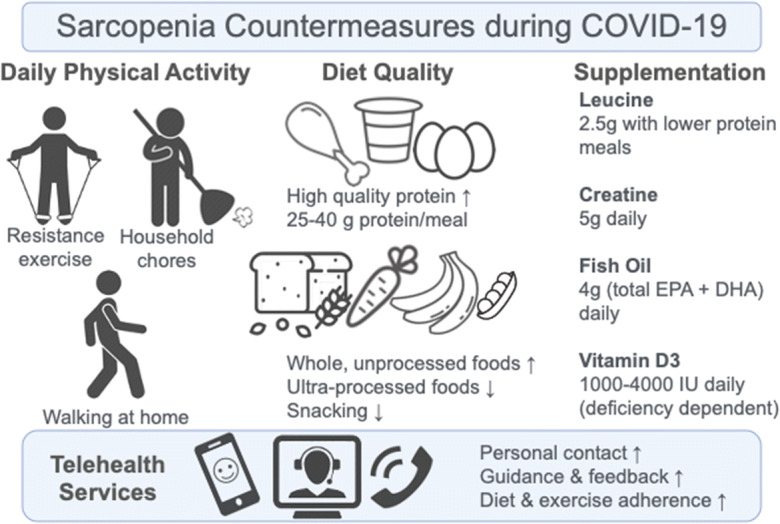
The COVID-19 pandemic is an extraordinary global emergency that has led to the implementation of unprecedented measures in order to stem the spread of the infection. Internationally, governments are enforcing measures such as travel bans, quarantine, isolation, and social distancing leading to an extended period of time at home. This has resulted in reductions in physical activity and changes in dietary intakes that have the potential to accelerate sarcopenia, a deterioration of muscle mass and function (more likely in older populations), as well as increases in body fat. These changes in body composition are associated with a number of chronic, lifestyle diseases including cardiovascular disease (CVD), diabetes, osteoporosis, frailty, cognitive decline, and depression. Furthermore, CVD, diabetes, and elevated body fat are associated with greater risk of COVID-19 infection and more severe symptomology, underscoring the importance of avoiding the development of such morbidities. Here we review mechanisms of sarcopenia and their relation to the current data on the effects of COVID-19 confinement on physical activity, dietary habits, sleep, and stress as well as extended bed rest due to COVID-19 hospitalization. The potential of these factors to lead to an increased likelihood of muscle loss and chronic disease will be discussed. By offering a number of home-based strategies including resistance exercise, higher protein intakes and supplementation, we can potentially guide public health authorities to avoid a lifestyle disease and rehabilitation crisis post-COVID-19. Such strategies may also serve as useful preventative measures for reducing the likelihood of sarcopenia in general and in the event of future periods of isolation.
Keywords: Appetite regulation; COVID-19; Inflammation; Obesity; Physical activity; Sarcopenia.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Geisler C, Braun W, Pourhassan M, Schweitzer L, Gluer CC, Bosy-Westphal A, et al. Gender-specific associations in age-related changes in resting energy expenditure (REE) and MRI measured body composition in healthy Caucasians. J Gerontol A Biol Sci Med Sci. 2016;71(7):941–946. - PubMed
-
- Scott D, de Courten B, Ebeling PR. Sarcopenia: a potential cause and consequence of type 2 diabetes in Australia’s ageing population? Med J Aust. 2016;205(7):329–333. - PubMed
-
- Bahat G, İlhan B. Sarcopenia and the cardiometabolic syndrome: a narrative review. Eur Geriatric Med. 2016;7(3):220–223.
-
- Xu W, Chen T, Cai Y, Hu Y, Fan L, Wu C. Sarcopenia in community-dwelling oldest old is associated with disability and poor physical function. J Nutr Health Aging. 2020;24(3):339–345. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
