

COVID-19 Trends Among School-Aged Children - United States, March 1-September 19, 2020
- PMID: 33001869
- PMCID: PMC7537558
- DOI: 10.15585/mmwr.mm6939e2
COVID-19 Trends Among School-Aged Children - United States, March 1-September 19, 2020
Erratum in
-
Erratum: Vol. 69, No. 39.MMWR Morb Mortal Wkly Rep. 2021 Jan 1;69(5152):1661-1662. doi: 10.15585/mmwr.mm695152a5. MMWR Morb Mortal Wkly Rep. 2021. PMID: 33382677 Free PMC article. No abstract available.
Abstract
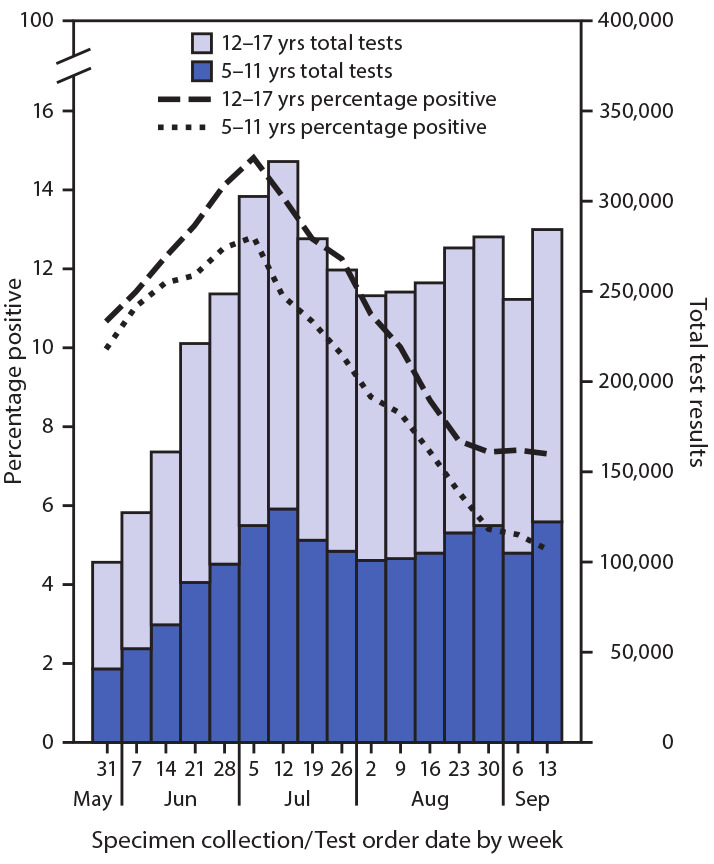
Approximately 56 million school-aged children (aged 5-17 years) resumed education in the United States in fall 2020.* Analysis of demographic characteristics, underlying conditions, clinical outcomes, and trends in weekly coronavirus disease 2019 (COVID-19) incidence during March 1-September 19, 2020 among 277,285 laboratory-confirmed cases in school-aged children in the United States might inform decisions about in-person learning and the timing and scaling of community mitigation measures. During May-September 2020, average weekly incidence (cases per 100,000 children) among adolescents aged 12-17 years (37.4) was approximately twice that of children aged 5-11 years (19.0). In addition, among school-aged children, COVID-19 indicators peaked during July 2020: weekly percentage of positive SARS-CoV-2 test results increased from 10% on May 31 to 14% on July 5; SARS-CoV-2 test volume increased from 100,081 tests on May 31 to 322,227 on July 12, and COVID-19 incidence increased from 13.8 per 100,000 on May 31 to 37.9 on July 19. During July and August, test volume and incidence decreased then plateaued; incidence decreased further during early September and might be increasing. Percentage of positive test results decreased during August and plateaued during September. Underlying conditions were more common among school-aged children with severe outcomes related to COVID-19: among school-aged children who were hospitalized, admitted to an intensive care unit (ICU), or who died, 16%, 27%, and 28%, respectively, had at least one underlying medical condition. Schools and communities can implement multiple, concurrent mitigation strategies and tailor communications to promote mitigation strategies to prevent COVID-19 spread. These results can provide a baseline for monitoring trends and evaluating mitigation strategies.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
