

Impact of PI-RADS Category 3 lesions on the diagnostic accuracy of MRI for detecting prostate cancer and the prevalence of prostate cancer within each PI-RADS category: A systematic review and meta-analysis
- PMID: 33002371
- PMCID: PMC7934301
- DOI: 10.1259/bjr.20191050
Impact of PI-RADS Category 3 lesions on the diagnostic accuracy of MRI for detecting prostate cancer and the prevalence of prostate cancer within each PI-RADS category: A systematic review and meta-analysis
Abstract
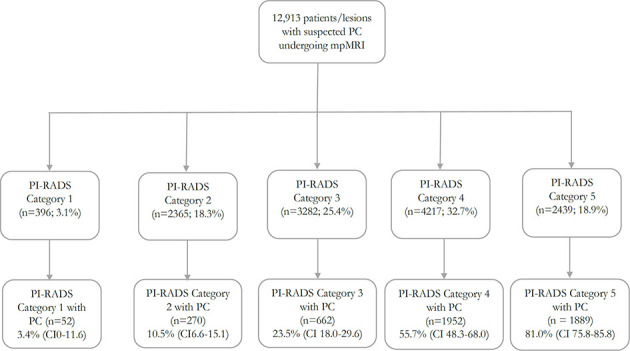
Objective: To evaluate Prostate Imaging Reporting and Data System (PI-RADS) category 3 lesions' impact on the diagnostic test accuracy (DTA) of MRI for prostate cancer (PC) and to derive the prevalence of PC within each PI-RADS category.
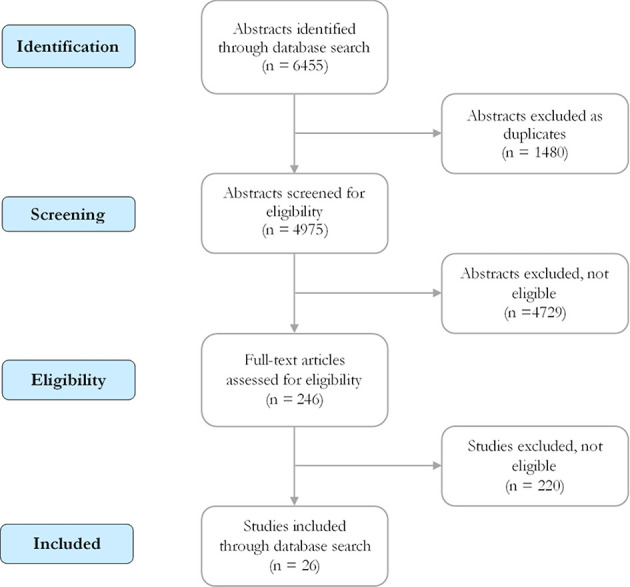
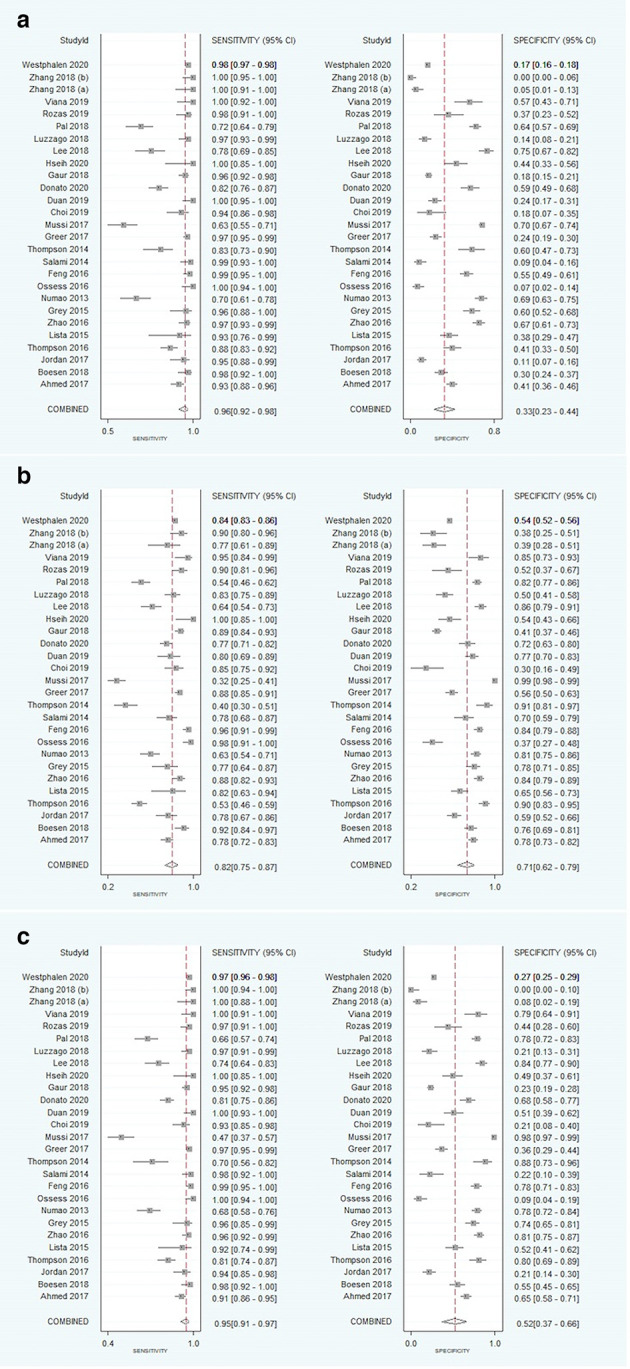
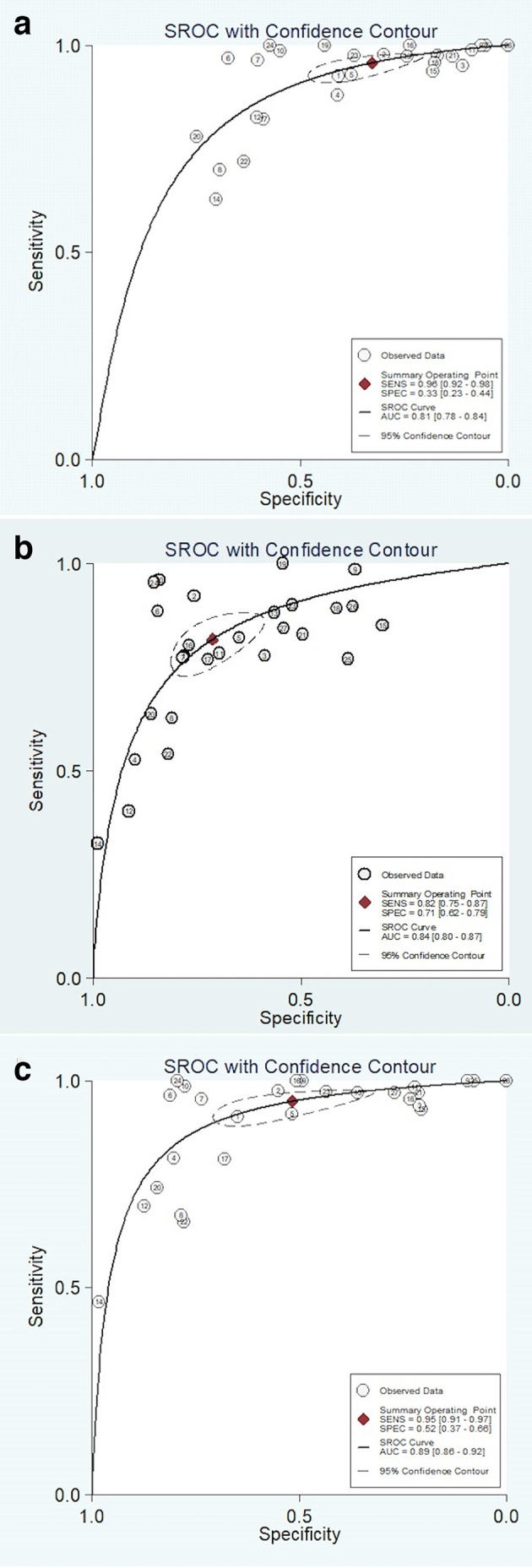
Methods: MEDLINE and Embase were searched until April 10, 2020 for studies reporting on the DTA of MRI by PI-RADS category. Accuracy metrics were calculated using a bivariate random-effects meta-analysis with PI-RADS three lesions treated as a positive test, negative test, and excluded from the analysis. Differences in DTA were assessed utilizing meta-regression. PC prevalence within each PI-RADS category was estimated with a proportional meta-analysis.
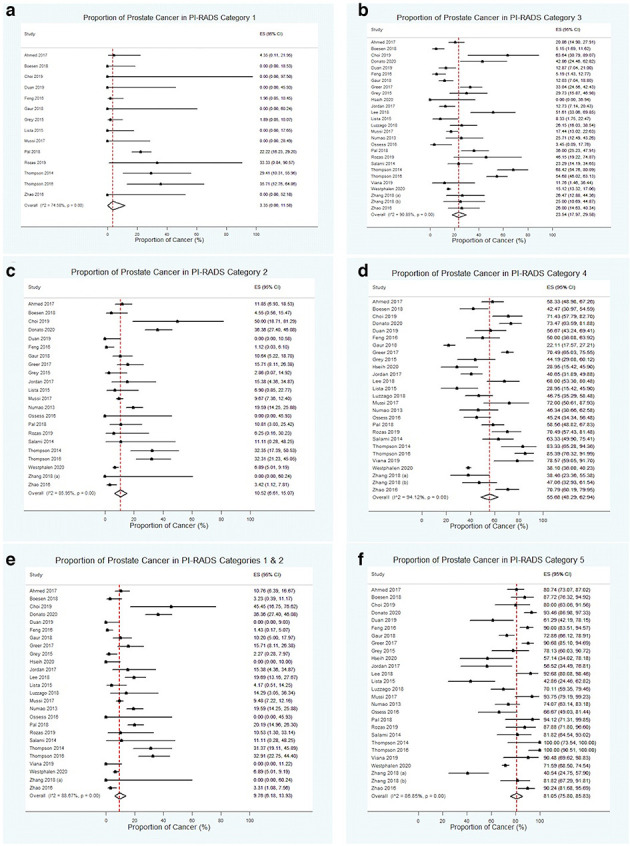
Results: In total, 26 studies reporting on 12,913 patients (4,853 with PC) were included. Sensitivities for PC in the positive, negative, and excluded test groups were 96% (95% confidence interval [CI] 92-98), 82% (CI 75-87), and 95% (CI 91-97), respectively. Specificities for the positive, negative, and excluded test groups were 33% (CI 23-44), 71% (CI 62-79), and 52% (CI 37-66), respectively. Meta-regression demonstrated higher sensitivity (p < 0.001) and lower specificity (p < 0.001) in the positive test group compared to the negative group. Clinically significant PC prevalences were 5.9% (CI 0-17.1), 11.4% (CI 6.5-17.3), 24.9% (CI 18.4-32.0), 55.7% (CI 47.8-63.5), and 81.4% (CI 75.9-86.4) for PI-RADS categories 1, 2, 3, 4 and 5, respectively.
Conclusion: PI-RADS category 3 lesions can significantly impact the DTA of MRI for PC detection. A low prevalence of clinically significant PC is noted in PI-RADS category 1 and 2 cases.
Advances in knowledge: Inclusion or exclusion of PI-RADS category 3 lesions impacts the DTA of MRI for PC detection.
Conflict of interest statement
Figures
References
-
- Mulhem E, Beaumont W, Heights S, Fulbright MN, Hospital P, Lyon S, et al. Prostate cancer screening. 2015;.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
