

Mitral valve repair for degenerative mitral regurgitation in patients with left ventricular systolic dysfunction: early and mid-term outcomes
- PMID: 33004041
- PMCID: PMC7528233
- DOI: 10.1186/s13019-020-01309-6
Mitral valve repair for degenerative mitral regurgitation in patients with left ventricular systolic dysfunction: early and mid-term outcomes
Abstract
Background: This study aims to evaluate the early and mid-term outcomes of mitral valve repair for degenerative mitral regurgitation (MR) in patients with left ventricular systolic dysfunction.
Methods: From January 2005 to December 2016, the profiles of patients with degenerative MR who underwent mitral valve repair at our institution were analyzed. Left ventricular systolic dysfunction was defined as an ejection fraction < 60% or left ventricular end-systolic dimension > 40 mm. Finally, 322 patients with left ventricular systolic dysfunction were included in this study. The prognosis of left ventricular function during follow-up was evaluated and preoperative factors associated with deteriorated left ventricular systolic function during follow-up were analyzed.
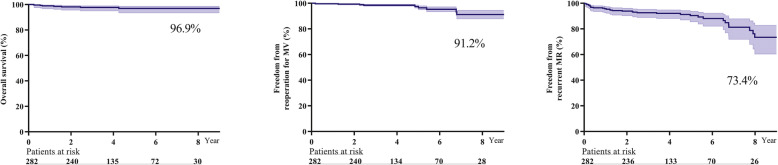
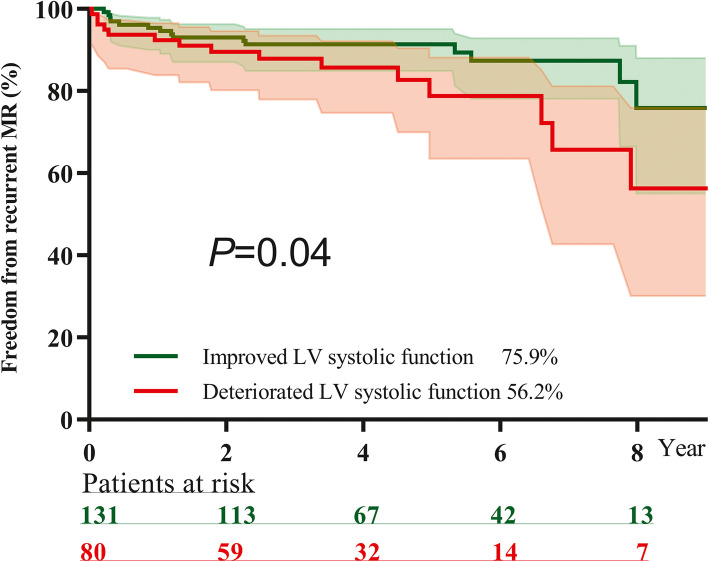
Results: The in-hospital mortality rate was 1.6%. The rate of eight-year overall survival, freedom from reoperation for mitral valve and freedom from recurrent MR were 96.9, 91.2 and 73.4%, respectively. Intraoperative residual mild MR (hazard ratio 4.82) and an isolated anterior leaflet lesion (hazard ratio 2.48) were independent predictive factors for recurrent MR. During follow-up, 212 patients underwent echocardiography examinations at our institution. Among them, 132 patients had improved left ventricular systolic function, and 80 patients had deteriorated left ventricular systolic. Freedom from recurrent MR was found in 75.9% of the improved left ventricular systolic function group and 56.2% of the deteriorated left ventricular systolic function group (P = 0.047). An age > 50 years (odds ratio 2.40), ejection fraction≤52% (odds ratio 2.79) and left ventricular end-systolic dimension≥45 mm (odds ratio 2.31) were independent risk factors for deteriorated left ventricular systolic function during follow-up.
Conclusions: Mitral valve repair could be safely performed for degenerative MR in patients with left ventricular systolic dysfunction. Intraoperative residual mild MR and an isolated anterior leaflet lesion were independent predictive factors for recurrent MR. An age > 50 years, ejection fraction≤52% and left ventricular end-systolic dimension≥45 mm were independent risk factors for deteriorated left ventricular systolic function during follow-up.
Keywords: Degenerative mitral regurgitation; Left ventricular systolic dysfunction; Mitral valve repair.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Barón-Esquivias G, Baumgartner H, et al. Guidelines on the management of valvular heart disease (version 2012): the joint task force on the management of Valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur J Cardiothorac Surg. 2012;42(4):S1–44. doi: 10.1093/ejcts/ezs455. - DOI - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, III, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129:e521–e643. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Fleisher LA, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the Management of Patients with Valvular Heart Disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2017;135(25):e1159–e1195. doi: 10.1161/CIR.0000000000000503. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
