

Implementation of lung protective ventilation order to improve adherence to low tidal volume ventilation: A RE-AIM evaluation
- PMID: 33004237
- PMCID: PMC7979571
- DOI: 10.1016/j.jcrc.2020.09.013
Implementation of lung protective ventilation order to improve adherence to low tidal volume ventilation: A RE-AIM evaluation
Abstract
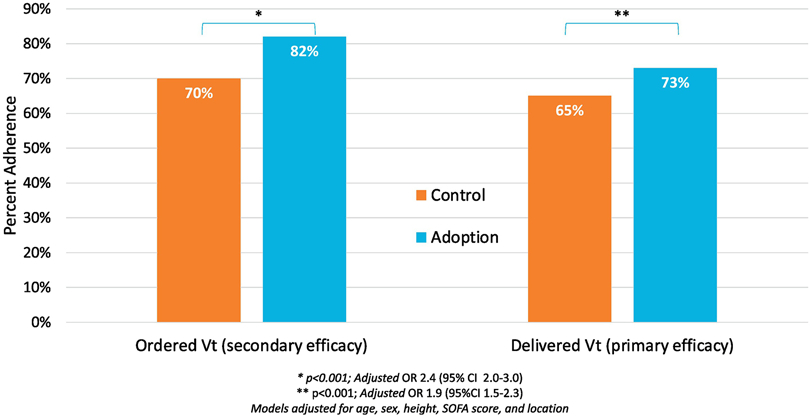
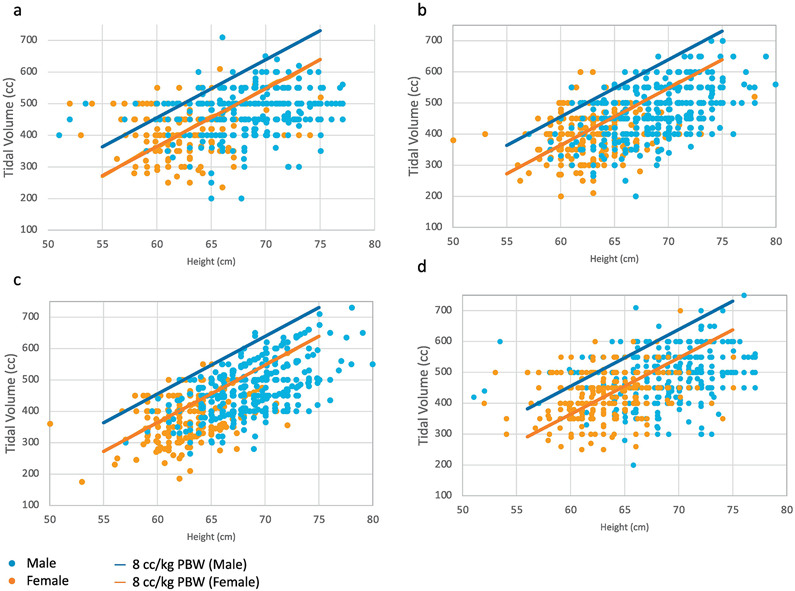
Purpose: Lung protective ventilation (LPV), defined as a tidal volume (Vt) ≤8 cc/kg of predicted body weight, reduces ventilator-induced lung injury but is applied inconsistently.
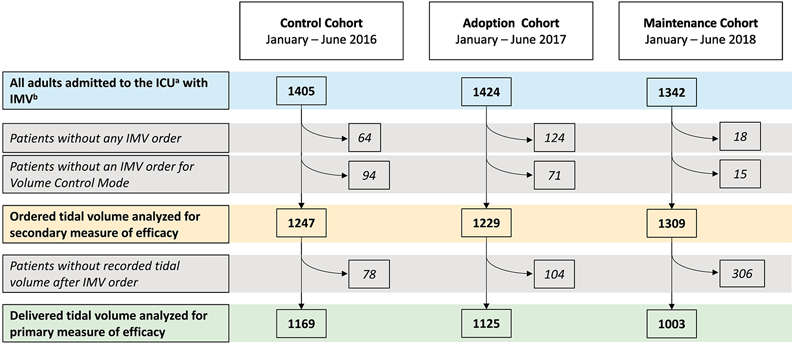
Materials and methods: We conducted a prospective, quasi-experimental, cohort study of adults mechanically ventilated admitted to intensive care units (ICU) in the year before, year after, and second year after implementation of an electronic medical record based LPV order, and a cross-sectional qualitative study of ICU providers regarding their perceptions of the order. We applied the Reach, Efficacy, Adoption, Implementation, and Maintenance (RE-AIM) framework to evaluate the implementation.
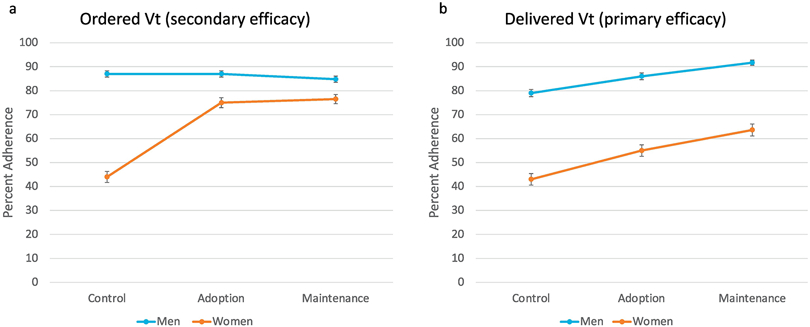
Results: There were 1405, 1424, and 1342 in the control, adoption, and maintenance cohorts, representing 95% of mechanically ventilated adult ICU patients. The overall prevalence of LPV increased from 65% to 73% (p < 0.001, adjusted-OR for LPV adherence: 1.9, 95% CI 1.5-2.3), but LPV adherence in women was approximately 30% worse than in men (women: 44% to 56% [p < 0.001],men: 79% to 86% [p < 0.001]). ICU providers noted difficulty obtaining an accurate height measurement and mistrust of the Vt calculation as barriers to implementation. LPV adherence increased further in the second year post implementation.
Conclusion: We designed and implemented an LPV order that sustainably improved LPV adherence across diverse ICUs.
Keywords: Clinical decision support tool (CDS); Implementation science; Low tidal volume ventilation (LTVV); Lung protective ventilation (LPV); Mechanical ventilation.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest There are no conflicts of interest or competing interest regarding this manuscript.
Figures
References
-
- Acute Respiratory Distress Syndrome N, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342: 1301–1308. - PubMed
-
- Needham DM, Yang T, Dinglas VD, Mendez-Tellez PA, Shanholtz C, Sevransky JE, Brower RG, Pronovost PJ, Colantuoni E. Timing of low tidal volume ventilation and intensive care unit mortality in acute respiratory distress syndrome. A prospective cohort study. Am J Respir Crit Care Med 2015; 191: 177–185. - PMC - PubMed
-
- Futier E, Constantin JM, Paugam-Burtz C, Pascal J, Eurin M, Neuschwander A, Marret E, Beaussier M, Gutton C, Lefrant JY, Allaouchiche B, Verzilli D, Leone M, De Jong A, Bazin JE, Pereira B, Jaber S, Group IS. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med 2013; 369: 428–437. - PubMed
-
- Neto AS, Simonis FD, Barbas CS, Biehl M, Determann RM, Elmer J, Friedman G, Gajic O, Goldstein JN, Linko R, Pinheiro de Oliveira R, Sundar S, Talmor D, Wolthuis EK, Gama de Abreu M, Pelosi P, Schultz MJ, Investigators PRVN. Lung-Protective Ventilation With Low Tidal Volumes and the Occurrence of Pulmonary Complications in Patients Without Acute Respiratory Distress Syndrome: A Systematic Review and Individual Patient Data Analysis. Crit Care Med 2015; 43: 2155–2163. - PubMed
-
- Bagga S, Paluzzi DE, Chen CY, Riggio JM, Nagaraja M, Marik PE, Baram M. Better ventilator settings using a computerized clinical tool. Respir Care 2014; 59: 1172–1177. - PubMed
