

Risk of complicated birth at term in nulliparous and multiparous women using routinely collected maternity data in England: cohort study
- PMID: 33004347
- PMCID: PMC7527835
- DOI: 10.1136/bmj.m3377
Risk of complicated birth at term in nulliparous and multiparous women using routinely collected maternity data in England: cohort study
Abstract
Objectives: To determine the rate of complicated birth at term in women classified at low risk according to the National Institute for Health and Care Excellence guideline for intrapartum care (no pre-existing medical conditions, important obstetric history, or complications during pregnancy) and to assess if the risk classification can be improved by considering parity and the number of risk factors.
Design: Cohort study using linked electronic maternity records.
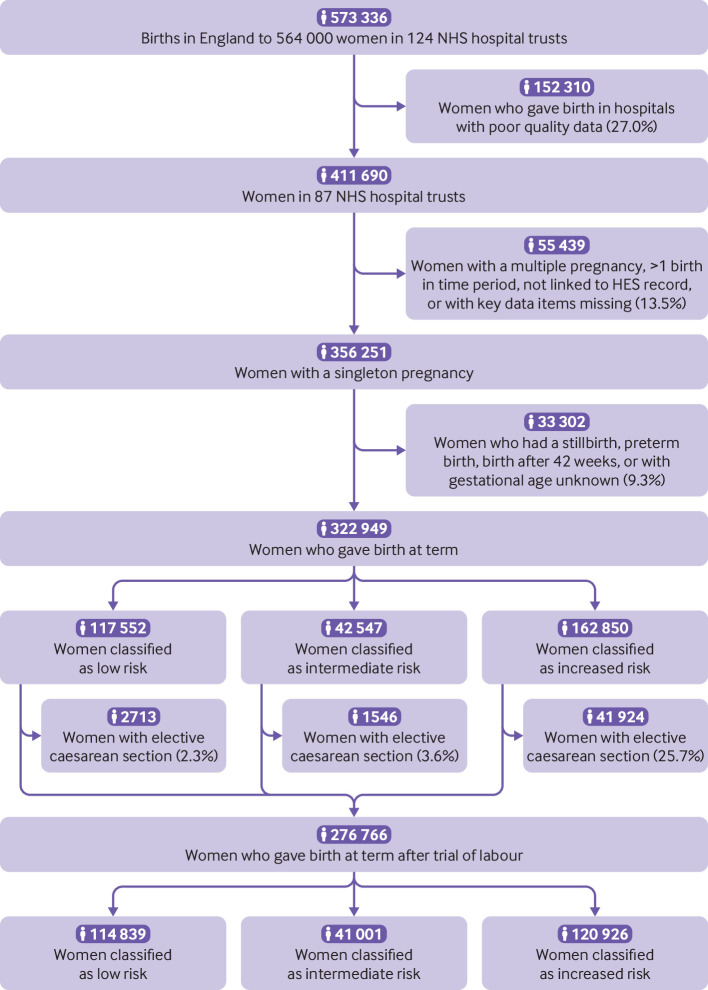
Participants: 276 766 women with a singleton birth at term after a trial of labour in 87 NHS hospital trusts in England between April 2015 and March 2016.
Main outcome measure: A composite outcome of complicated birth, defined as a birth with use of an instrument, caesarean delivery, anal sphincter injury, postpartum haemorrhage, or Apgar score of 7 or less at five minutes.
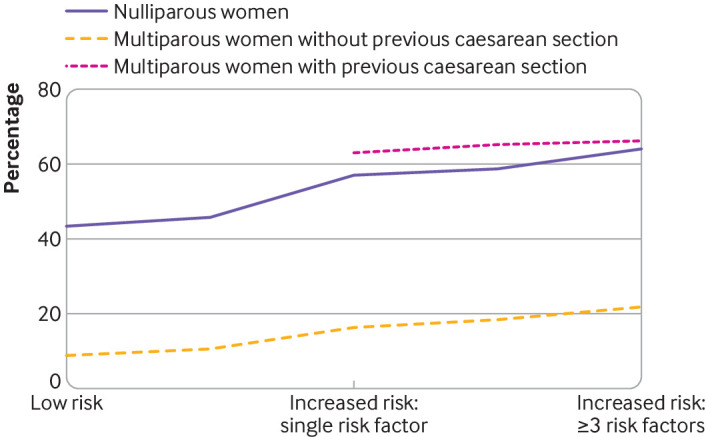
Results: Multiparous women without a history of caesarean section had the lowest rates of complicated birth, varying from 8.8% (4879 of 55 426 women, 95% confidence interval 8.6% to 9.0%) in those without specific risk factors to 21.8% (613 of 2811 women, 20.2% to 23.4%) in those with three or more. The rate of complicated birth was higher in nulliparous women, with corresponding rates varying from 43.4% (25 805 of 59 413 women, 43.0% to 43.8%) to 64.3% (364 of 566 women, 60.3% to 68.3%); and highest in multiparous women with previous caesarean section, with corresponding rates varying from 42.9% (3426 of 7993 women, 41.8% to 44.0%) to 66.3% (554 of 836 women, 63.0% to 69.5%).
Conclusions: Nulliparous women without risk factors have substantially higher rates of complicated birth than multiparous women without a previous caesarean section even if the latter have multiple risk factors. Grouping women first according to parity and previous mode of birth, and then within these groups according to presence of specific risk factors would provide greater and more informed choice to women, better targeting of interventions, and fewer transfers during labour than according to the presence of risk factors alone.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: all individuals are or have been partially or wholly funded by the Healthcare Quality Improvement Partnership for their contribution to the submitted work. DP is also funded by Tommy’s Charity. All authors also declare no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. Dr Hawdon reports personal fees from expert medicolegal reporting, for defendant and claimant, on perinatal injury cases. The authors report no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- World Health Organization. WHO recommendations: intrapartum care for a positive childbirth experience. 2018. www.who.int/reproductivehealth/publications/intrapartum-care-guidelines/en/ - PubMed
-
- National Institute for Health and Care Excellence. Clinical Guideline 190: Intrapartum care for healthy women and babies 2014. nice.org.uk/guidance/cg190. - PubMed
-
- Hollowell J, Li Y, Bunch K, Brocklehurst P. A comparison of intrapartum interventions and adverse outcomes by parity in planned freestanding midwifery unit and alongside midwifery unit births: secondary analysis of ‘low risk’ births in the birthplace in England cohort. BMC Pregnancy Childbirth 2017;17:95. 10.1186/s12884-017-1271-2. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous