

A microstructural neural network biomarker for dystonia diagnosis identified by a DystoniaNet deep learning platform
- PMID: 33004625
- PMCID: PMC7586425
- DOI: 10.1073/pnas.2009165117
A microstructural neural network biomarker for dystonia diagnosis identified by a DystoniaNet deep learning platform
Abstract
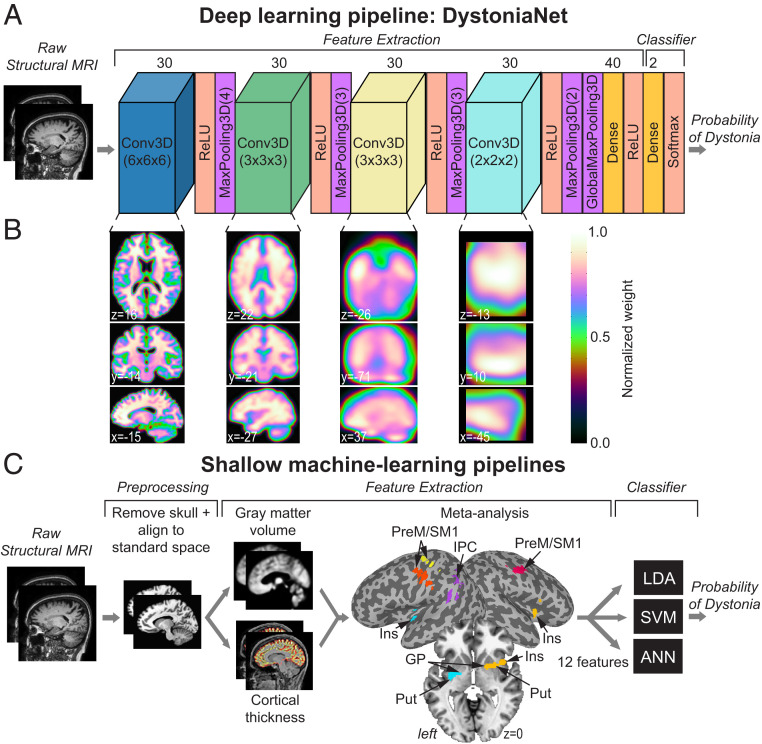
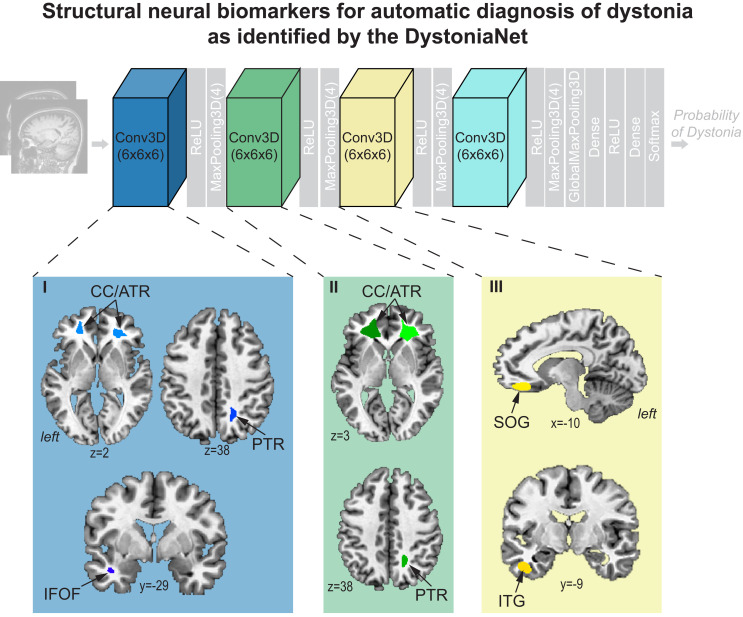
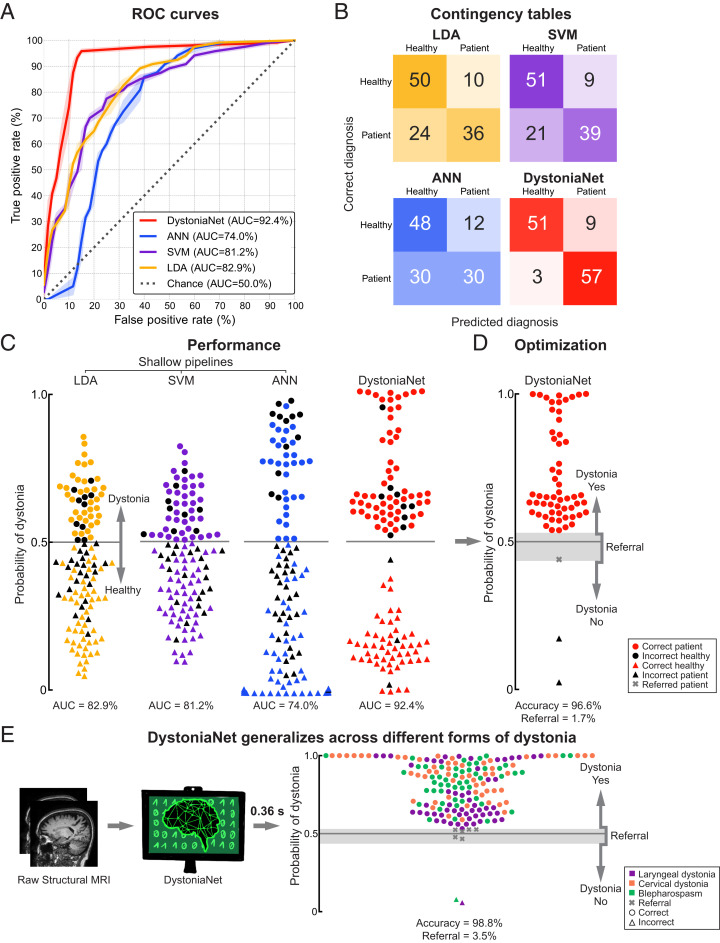
Isolated dystonia is a neurological disorder of heterogeneous pathophysiology, which causes involuntary muscle contractions leading to abnormal movements and postures. Its diagnosis is remarkably challenging due to the absence of a biomarker or gold standard diagnostic test. This leads to a low agreement between clinicians, with up to 50% of cases being misdiagnosed and diagnostic delays extending up to 10.1 y. We developed a deep learning algorithmic platform, DystoniaNet, to automatically identify and validate a microstructural neural network biomarker for dystonia diagnosis from raw structural brain MRIs of 612 subjects, including 392 patients with three different forms of isolated focal dystonia and 220 healthy controls. DystoniaNet identified clusters in corpus callosum, anterior and posterior thalamic radiations, inferior fronto-occipital fasciculus, and inferior temporal and superior orbital gyri as the biomarker components. These regions are known to contribute to abnormal interhemispheric information transfer, heteromodal sensorimotor processing, and executive control of motor commands in dystonia pathophysiology. The DystoniaNet-based biomarker showed an overall accuracy of 98.8% in diagnosing dystonia, with a referral of 3.5% of cases due to diagnostic uncertainty. The diagnostic decision by DystoniaNet was computed in 0.36 s per subject. DystoniaNet significantly outperformed shallow machine-learning algorithms in benchmark comparisons, showing nearly a 20% increase in its diagnostic performance. Importantly, the microstructural neural network biomarker and its DystoniaNet platform showed substantial improvement over the current 34% agreement on dystonia diagnosis between clinicians. The translational potential of this biomarker is in its highly accurate, interpretable, and generalizable performance for enhanced clinical decision-making.
Keywords: biomarker; brain MRI; dystonia; machine learning.
Copyright © 2020 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Hellberg C., Alinder E., Jaraj D., Puschmann A., Nationwide prevalence of primary dystonia, progressive ataxia and hereditary spastic paraplegia. Parkinsonism Relat. Disord. 69, 79–84 (2019). - PubMed
-
- Defazio G. et al., The Italian dystonia registry: Rationale, design and preliminary findings. Neurol. Sci. 38, 819–825 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
