

Sclerostin antibody stimulates periodontal regeneration in large alveolar bone defects
- PMID: 33004873
- PMCID: PMC7530715
- DOI: 10.1038/s41598-020-73026-y
Sclerostin antibody stimulates periodontal regeneration in large alveolar bone defects
Abstract
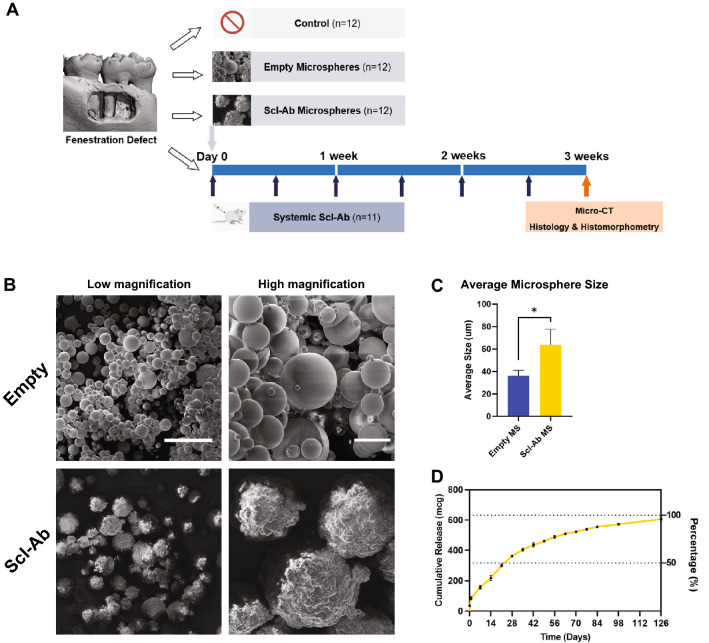
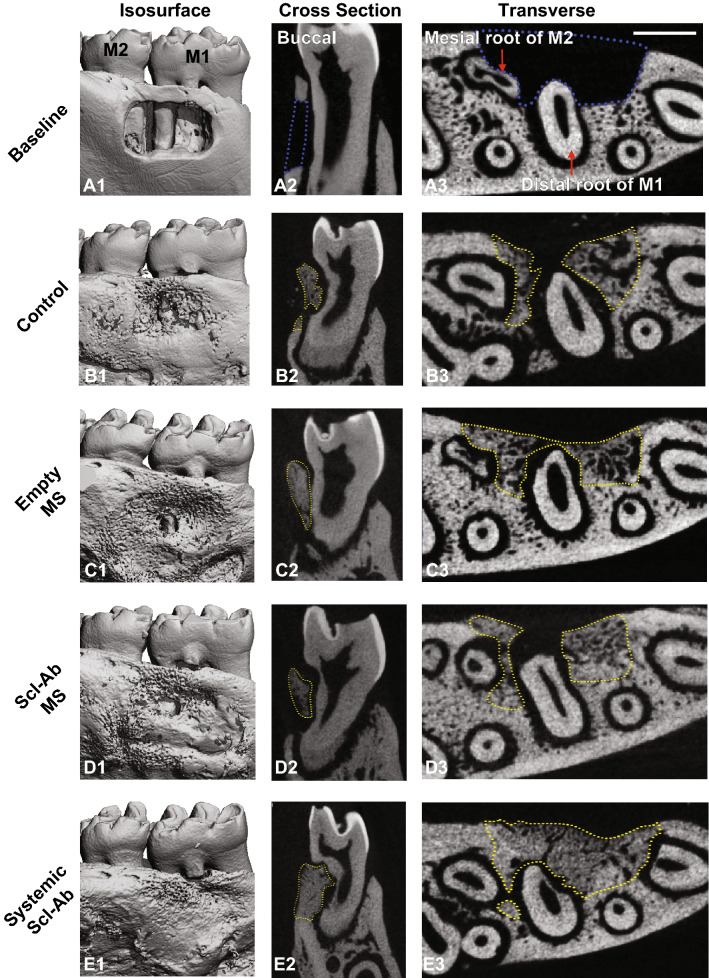
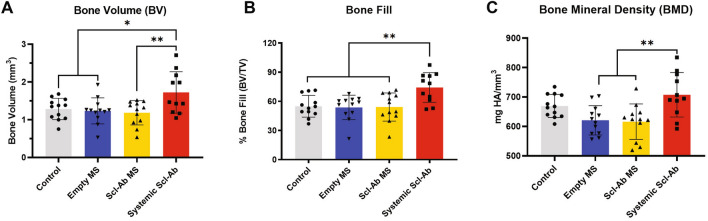
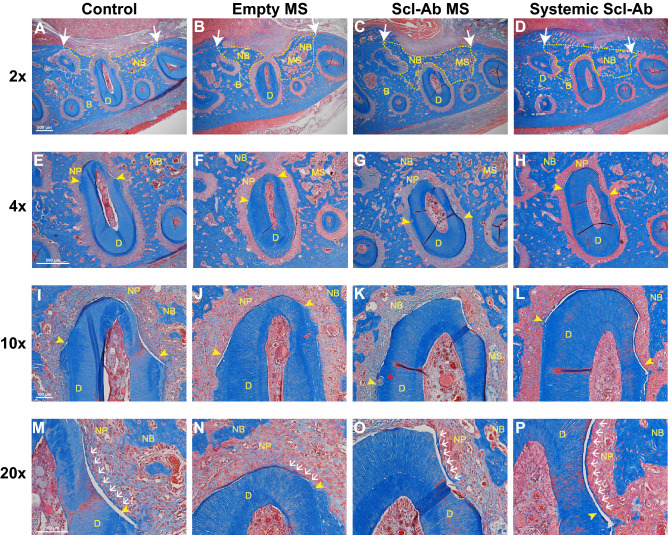
Destruction of the alveolar bone in the jaws can occur due to periodontitis, trauma or following tumor resection. Common reconstructive therapy can include the use of bone grafts with limited predictability and efficacy. Romosozumab, approved by the FDA in 2019, is a humanized sclerostin-neutralizing antibody (Scl-Ab) indicated in postmenopausal women with osteoporosis at high risk for fracture. Preclinical models show that Scl-Ab administration preserves bone volume during periodontal disease, repairs bone defects surrounding dental implants, and reverses alveolar bone loss following extraction socket remodeling. To date, there are no studies evaluating Scl-Ab to repair osseous defects around teeth or to identify the efficacy of locally-delivered Scl-Ab for targeted drug delivery. In this investigation, the use of systemically-delivered versus low dose locally-delivered Scl-Ab via poly(lactic-co-glycolic) acid (PLGA) microspheres (MSs) was compared at experimentally-created alveolar bone defects in rats. Systemic Scl-Ab administration improved bone regeneration and tended to increase cementogenesis measured by histology and microcomputed tomography, while Scl-Ab delivered by MSs did not result in enhancements in bone or cemental repair compared to MSs alone or control. In conclusion, systemic administration of Scl-Ab promotes bone and cemental regeneration while local, low dose delivery did not heal periodontal osseous defects in this study.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
