

Evidence of cortical thickness reduction and disconnection in high myopia
- PMID: 33004887
- PMCID: PMC7530748
- DOI: 10.1038/s41598-020-73415-3
Evidence of cortical thickness reduction and disconnection in high myopia
Abstract
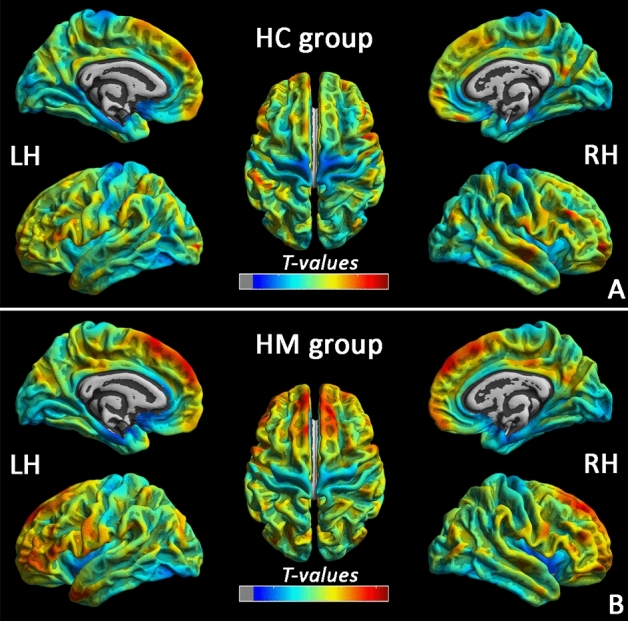
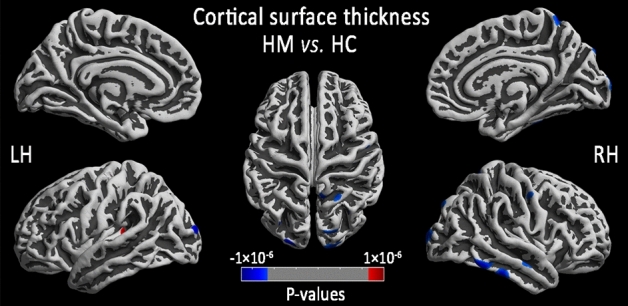
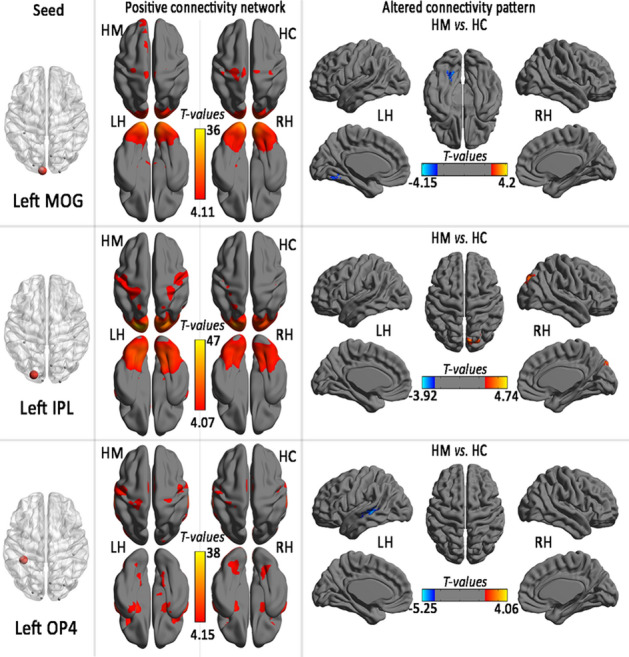
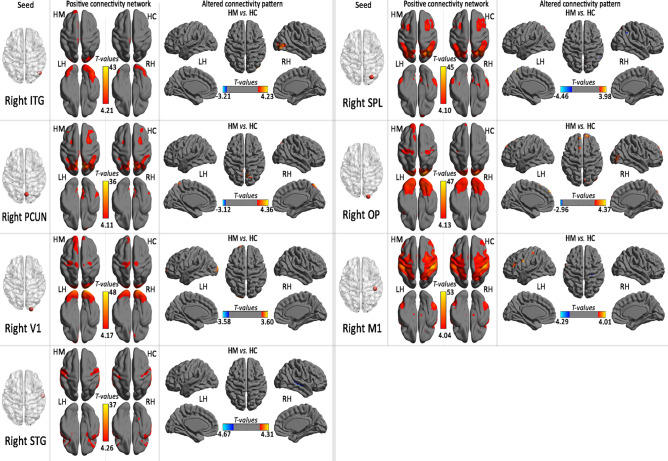
High myopia (HM) is associated with impaired long-distance vision. accumulating evidences reported that abnormal visual experience leads to dysfunction in brain activity in HM even corrected. However, whether the long-term of abnormal visual experience lead to neuroanatomical changes remain unknown, the aim at this study is to investigate the alternation of cortical surface thickness in HM patients. 82 patients with HM (HM groups), 57 healthy controls (HC groups) were recruited. All participants underwent high-resolution T1 and resting-state functional magnetic resonance imaging (MRI) scans. The cortical thickness analysis was preformed to investigate the neuroanatomical changes in HM patients using computational anatomy toolbox (CAT 12) toolbox. Compare with HCs, HM patients showed decreased the cortical surface thickness in the left middle occipital gyrus (MOG), left inferior parietal lobule (IPL), right inferior temporal gyrus (ITG), right precuneus, right primary visual area 1 (V1), right superior temporal gyrus (STG), right superior parietal lobule (SPL), right occipital pole, and right the primary motor cortex (M1), and increased to the parietal operculum (OP4) (P < 0.01, FWE-corrected), the mean cortical thickness of right orbitofrontal cortex (OFC), right dorsolateral prefrontal cortex (DLPFC) and right subcallosal cortex showed negatively correlation between clinical variables (axis length (ALM), the average macular thickness (AMT), keratometer (KER) 1, KER2, the mean KER, the mean macular fovea thickness (MFK), the refractive diopter) in HM patients. Our result mainly provided an evidence of cortical thickness reduction and disconnection in visual center and visual processing area, and cortical thickness increase in left multimodal integration region in HM patients. This may provide important significance of the study of the neural mechanism of HM.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Altered whole-brain gray matter volume in high myopia patients: a voxel-based morphometry study.Neuroreport. 2018 Jun 13;29(9):760-767. doi: 10.1097/WNR.0000000000001028. Neuroreport. 2018. PMID: 29634585 Free PMC article.
-
Cortical Surface Thickness in the Middle-Aged Brain with White Matter Hyperintense Lesions.Front Aging Neurosci. 2017 Jul 17;9:225. doi: 10.3389/fnagi.2017.00225. eCollection 2017. Front Aging Neurosci. 2017. PMID: 28769784 Free PMC article.
-
Altered grey matter volume and cortical thickness in patients with schizo-obsessive comorbidity.Psychiatry Res Neuroimaging. 2018 Jun 30;276:65-72. doi: 10.1016/j.pscychresns.2018.03.009. Epub 2018 Mar 28. Psychiatry Res Neuroimaging. 2018. PMID: 29628272
-
Neurovascular coupling dysfunction in high myopia patients: Evidence from a multi-modal magnetic resonance imaging analysis.J Neuroradiol. 2024 May;51(3):281-289. doi: 10.1016/j.neurad.2023.09.005. Epub 2023 Sep 29. J Neuroradiol. 2024. PMID: 37777086
-
Understanding how the immune system environment is controlled in high myopia cases.Int Immunopharmacol. 2024 Dec 25;143(Pt 1):113138. doi: 10.1016/j.intimp.2024.113138. Epub 2024 Oct 2. Int Immunopharmacol. 2024. PMID: 39362012 Review.
Cited by
-
Exploration of abnormal dynamic spontaneous brain activity in patients with high myopia via dynamic regional homogeneity analysis.Front Hum Neurosci. 2022 Aug 5;16:959523. doi: 10.3389/fnhum.2022.959523. eCollection 2022. Front Hum Neurosci. 2022. PMID: 35992950 Free PMC article.
-
Meridional Anisotropy of Foveal and Peripheral Resolution Acuity in Adults With Emmetropia, Myopia, and Astigmatism.Invest Ophthalmol Vis Sci. 2021 Aug 2;62(10):11. doi: 10.1167/iovs.62.10.11. Invest Ophthalmol Vis Sci. 2021. PMID: 34379095 Free PMC article.
-
Associations Between Myopia and Brain Volumes: An Observational and Genetic Analysis.Invest Ophthalmol Vis Sci. 2025 Jun 2;66(6):57. doi: 10.1167/iovs.66.6.57. Invest Ophthalmol Vis Sci. 2025. PMID: 40530922 Free PMC article.
-
Reorganized Brain Functional Network Topology in Presbycusis.Front Aging Neurosci. 2022 May 26;14:905487. doi: 10.3389/fnagi.2022.905487. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35693344 Free PMC article.
-
Spontaneous changes in brain network centrality in patients with pathological myopia: A voxel-wise degree centrality analysis.CNS Neurosci Ther. 2023 Aug;29(8):2186-2192. doi: 10.1111/cns.14168. Epub 2023 Mar 21. CNS Neurosci Ther. 2023. PMID: 36942490 Free PMC article.
References
-
- Wong YL, Saw SM. Epidemiology of pathologic myopia in asia and worldwide. Asia Pac. J. Ophthalmol. (Phila). 2016;5:394–402. - PubMed
-
- Jonas JB, Xu L, Wei WB, Wang YX, Jiang WJ. Myopia in China: a populationbased cross-sectional, histological, and experimental study. Lancet. 2016;388:S20.
-
- Margherio, R. R. & Schepens, C. L. Macular breaks. 1. Diagnosis, etiology, and observations. Am J Ophthalmol. 74, 219–232 (1972). - PubMed
-
- Zhai L, et al. Altered functional connectivity density in high myopia. Behav Brain Res. 2016;303:85–92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
