

Detection rate of diabetic macular microaneurysms comparing dye-based angiography and optical coherence tomography angiography
- PMID: 33005009
- PMCID: PMC7530679
- DOI: 10.1038/s41598-020-73516-z
Detection rate of diabetic macular microaneurysms comparing dye-based angiography and optical coherence tomography angiography
Abstract
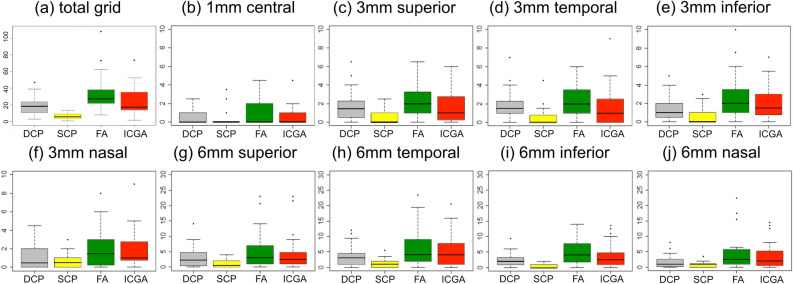
Diabetic maculopathy (DM) is a microvascular dysfunction clinically characterized by microaneurysms (MA) leading to edema and central visual deprivation. This prospective explorative study investigated 27 eyes of 17 patients with DM by fluorescein/indocyanine green angiography (FA/ICGA; SPECTRALIS HRA-OCT, Heidelberg Engineering) and by swept source-optical coherence tomography angiography (SS-OCTA; DRI-OCT Triton Plus, Topcon) to identify clinically relevant MAs. The SS-OCTA cubes were split into the superficial capillary plexus (SCP) and the deep capillary plexus (DCP) according to the automated segmentation. The images of all modalities were superimposed for alignment by an Early Treatment Diabetic Retinopathy Study grid overlay and compared to each other. In total, the mean number of MAs in FA was 33.4 ± 22 (standard deviation) (median 27.5 [q1:21.75;q3:38.25]), in ICGA 24.9 ± 16.9 (17.5 [14;35]), in the SCP 6.5 ± 3.7 (5.5 [3.75;9.25]) and in the DCP 18.1 ± 10.5 (18.5 [10.75;23.5]). Mixed effects models between ICGA and the DCP were borderline significant (p = 0.048; 95% confidence interval 0.21 to 13.49), whereas all other imaging methods differed significantly. Quantitative analysis of MAs in DM showed a plausible agreement between ICGA and the DCP in SS-OCTA. These findings contribute to the imaging methodology in DM.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
