

Urgent Airway Management and Postoperative Complications in a Patient with Trichorhinophalangeal Syndrome
- PMID: 33005456
- PMCID: PMC7509557
- DOI: 10.1155/2020/8835533
Urgent Airway Management and Postoperative Complications in a Patient with Trichorhinophalangeal Syndrome
Abstract
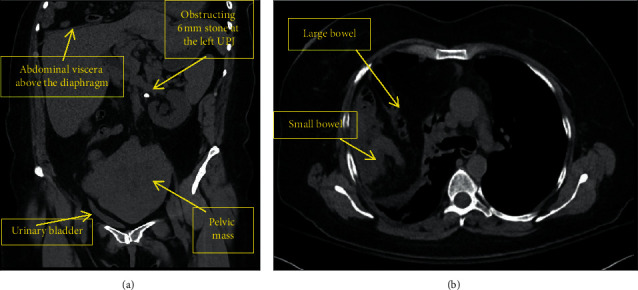
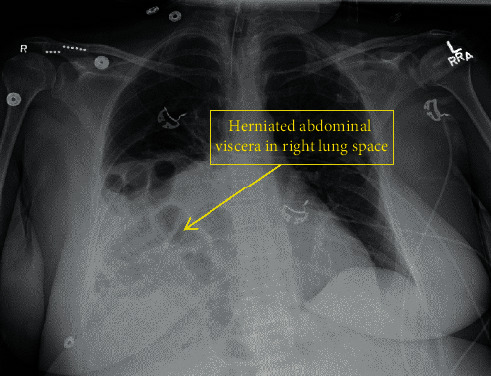
Trichorhinophalangeal syndrome (TRPS) is a genetic disorder that may pose anesthetic challenges. We present a case of airway management for urgent surgery in a 56-year-old female with TRPS and difficult airway (macroglossia, narrow glottic opening, and hypoplastic epiglottis). Intubation was successful with video laryngoscopy using a size 2.5 pediatric blade and size 5.0 endotracheal tube. During emergence, she experienced bronchospasm and persistent urosepsis, necessitating intensive care unit (ICU) admission. Her pulmonary reserve was hindered by a Morgagni hernia causing lung compression. Our case demonstrates challenges in TRPS including challenging airway, decreased pulmonary reserve, and joint laxity introducing potential for spinal cord injury.
Copyright © 2020 Sarvie Esmaeilzadeh et al.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Adam M. P., Ardinger H. H., Pagon R. A., et al. Trichorhinophalangeal Syndrome. GeneReviews. Bethesda, MD, USA: National Center for Biotechnology Information; 1993.
-
- Hall B. D., Langer L. O., Giedion A., et al. Langer-Giedion syndrome. Birth Defects Original Article Series. 1974;10(12):147–164. - PubMed
-
- Lu F. L., Hou J. W., Tsai W. S., Teng R. J., Yau K. I., Wang T. R. Tricho-rhino-phalangeal syndrome type II associated with epiglottic aplasia and congenital nephrotic syndrome. Journal of the Formosan Medical Association = Taiwan Yi Zhi. 1997;96(3):217–221. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
