

Cardiogenic shock and acute kidney injury: the rule rather than the exception
- PMID: 33006038
- PMCID: PMC8024234
- DOI: 10.1007/s10741-020-10034-0
Cardiogenic shock and acute kidney injury: the rule rather than the exception
Abstract
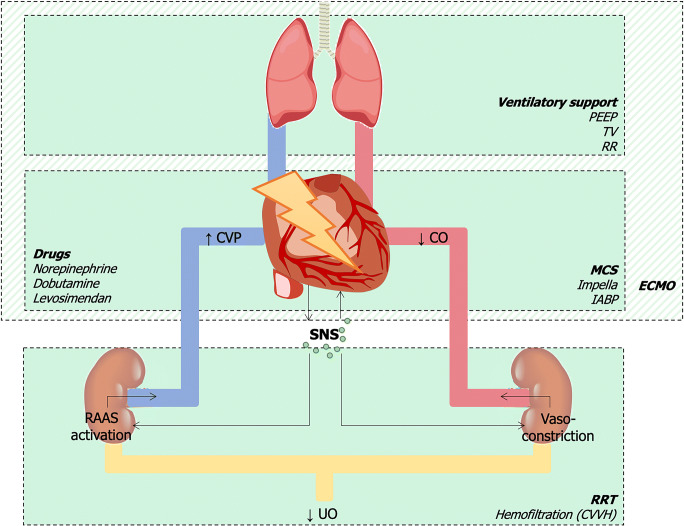
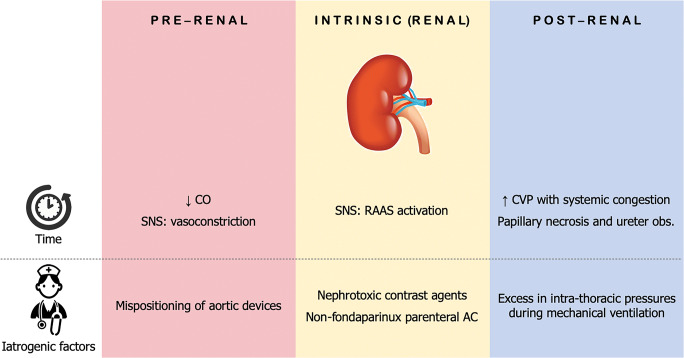
Cardiogenic shock (CS) is a life-threatening condition of poor end-organ perfusion, caused by any cardiovascular disease resulting in a severe depression of cardiac output. Despite recent advances in replacement therapies, the outcome of CS is still poor, and its management depends more on empirical decisions rather than on evidence-based strategies. By its side, acute kidney injury (AKI) is a frequent complication of CS, resulting in the onset of a cardiorenal syndrome. The combination of CS with AKI depicts a worse clinical scenario and holds a worse prognosis. Many factors can lead to acute renal impairment in the setting of CS, either for natural disease progression or for iatrogenic causes. This review aims at collecting the current evidence-based acknowledgments in epidemiology, pathophysiology, clinical features, diagnosis, and management of CS with AKI. We also attempted to highlight the major gaps in evidence as well as to point out possible strategies to improve the outcome.
Keywords: Acute kidney injury; Cardiogenic shock; Heart failure; Outcome; Replacement therapy.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, Thiele H, Washam JB, Cohen MG, American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Mission: Lifeline Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136:e232–e268. - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, Picard MH, Menegus MA, Boland J, Dzavik V, Thompson CR, Wong SC, Steingart R, Forman R, Aylward PE, Godfrey E, Desvigne-Nickens P, LeJemtel TH. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med. 1999;341:625–634. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
-
- Chua HR, Glassford N, Bellomo R. Acute kidney injury after cardiac arrest. Resuscitation. 2012;83:721–727. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
