

Type A aortic dissection in aneurysms having modelled pre-dissection maximum diameter below 45 mm: should we implement current guidelines to improve the survival benefit of prophylactic surgery?
- PMID: 33006606
- PMCID: PMC7850065
- DOI: 10.1093/ejcts/ezaa351
Type A aortic dissection in aneurysms having modelled pre-dissection maximum diameter below 45 mm: should we implement current guidelines to improve the survival benefit of prophylactic surgery?
Abstract
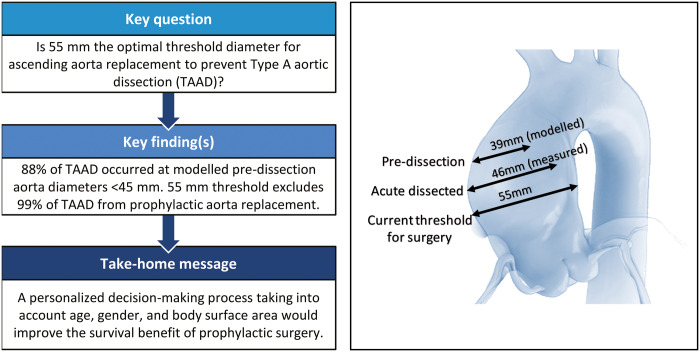
Objectives: Current guidelines recommend prophylactic replacement of the ascending aorta at an aneurysmal diameter of >55 mm to prevent acute Type A aortic dissection (TAAD) in non-Marfan patients. Several publications have challenged this threshold, suggesting that surgery should be performed in smaller aneurysms to prevent this devastating disease. We reviewed our experience with measuring aortic size at the time of TAAD to validate the existing recommendation for prophylactic ascending aorta replacement.
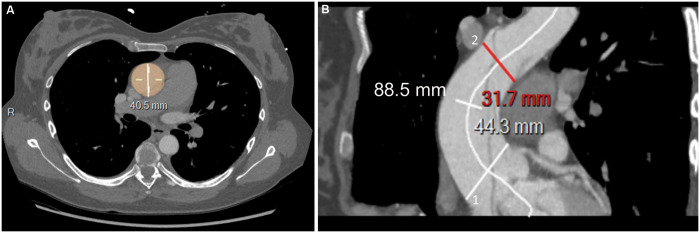
Methods: All patients who had been admitted for TAAD to our emergency department from 2014 to 2019 and underwent ascending aorta replacement were included. Marfan patients were excluded. The maximum diameter of the dissected aorta was measured preoperatively using CT scan. We estimated the aortic diameter at the time of dissection to be 7 mm smaller than the measured maximum diameter of the dissected aorta (modelled pre-dissection diameter).
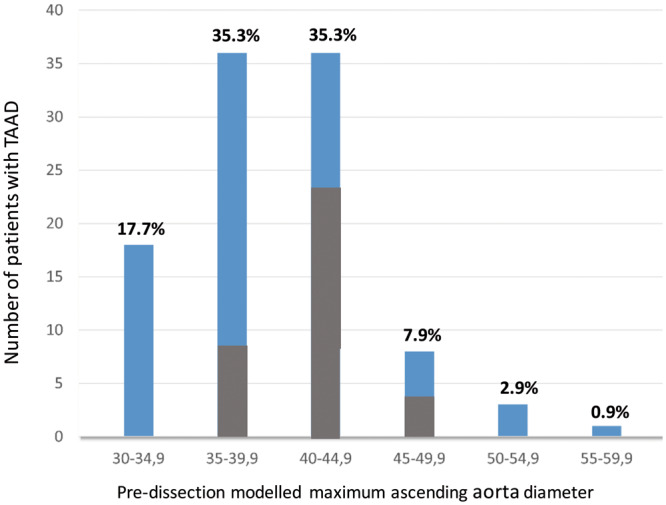
Results: Overall, 102 patients were included. Of these, 67 were male (65.6%) and 35 were female (34.4%), and the cohort's mean age was 65 ± 12.1 years. In addition, 66% were treated for arterial hypertension. The mean maximum modelled pre-dissection diameter was 39.6 ± 4.8 mm: 39.1 ± 5.1 mm in men and 40.7 ± 2.8 mm in women (P = 0.1). The cumulative 30-day mortality rate was 19.6% (20/102).
Conclusions: TAAD occurred at a modelled aortic diameter below 45 mm in 87.7% of our patients. Therefore, the current aortic diameter threshold of 55 mm excludes ∼99% of patients with TAAD from prophylactic replacement of the ascending aorta. The maximum diameter of the ascending aorta warrants reappraisal and this parameter should be a distinct part of a personalized decision-making process that also takes into account age, gender and body surface area to establish the surgical indication for preventive aorta replacement aimed to improve the survival benefit of this procedure.
Keywords: Acute aortic syndrome; Aortic aneurysm; Aortic dissection; Aortic surgery.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Comment in
-
Challenging the threshold for prophylactic surgery in aneurysms of the ascending aorta.Eur J Cardiothorac Surg. 2021 Jul 14;60(1):202. doi: 10.1093/ejcts/ezaa448. Eur J Cardiothorac Surg. 2021. PMID: 33279993 No abstract available.
-
Reply to Greco and Demertzis.Eur J Cardiothorac Surg. 2021 Jul 14;60(1):202-203. doi: 10.1093/ejcts/ezaa449. Eur J Cardiothorac Surg. 2021. PMID: 33280044 No abstract available.
-
Reply to Peterss et al.Eur J Cardiothorac Surg. 2022 Feb 18;61(3):731-732. doi: 10.1093/ejcts/ezab354. Eur J Cardiothorac Surg. 2022. PMID: 34347051 No abstract available.
-
What do we know? The dilemma of modelling risk for aortic dissection.Eur J Cardiothorac Surg. 2022 Feb 18;61(3):731. doi: 10.1093/ejcts/ezab361. Eur J Cardiothorac Surg. 2022. PMID: 34347075 No abstract available.
References
-
- Mészáros I, Mórocz J, Szlávi J, Schmidt J, Tornóci L, Nagy L et al. Epidemiology and clinicopathology of aortic dissection. Chest 2000;117:1271–8. - PubMed
-
- Abe T, Yamamoto H, Miyata H, Miyata H, Motomura N, Tokuda Y et al. Patient trends and outcomes of surgery for type A acute aortic dissection in Japan: an analysis of more than 10 000 patients from the Japan Cardiovascular Surgery Database. Eur J CardioThorac Surg 2020;57:660–7. - PubMed
-
- Erbel R, Aboyans V, Boileau C, Bossone E, Di Bartolomeo R, Eggebrecht H et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). ESC Committee for Practice Guidelines. Eur Heart J 2014. 1;35:2873–926. - PubMed
-
- Coady MA1, Rizzo JA, Hammond GL, Mandapati D, Darr U, Kopf GS et al. What is the appropriate size criterion for resection of thoracic aortic aneurysms? J Thorac Cardiovasc Surg 1997;113:476–91. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
