

Pre-operative aerobic exercise on metabolic health and surgical outcomes in patients receiving bariatric surgery: A pilot trial
- PMID: 33006980
- PMCID: PMC7531806
- DOI: 10.1371/journal.pone.0239130
Pre-operative aerobic exercise on metabolic health and surgical outcomes in patients receiving bariatric surgery: A pilot trial
Abstract
Objective: Examine if adding aerobic exercise to standard medical care (EX+SC) prior to bariatric surgery improves metabolic health in relation to surgical outcomes.
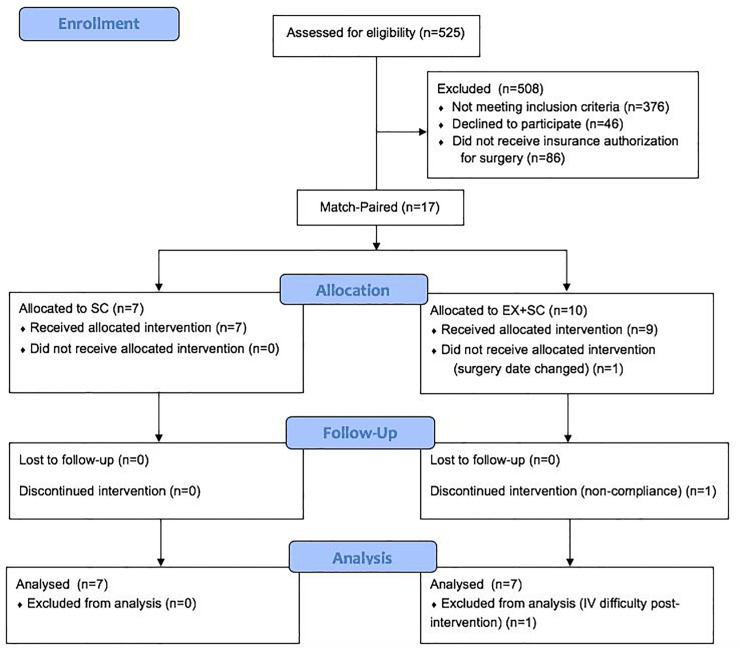
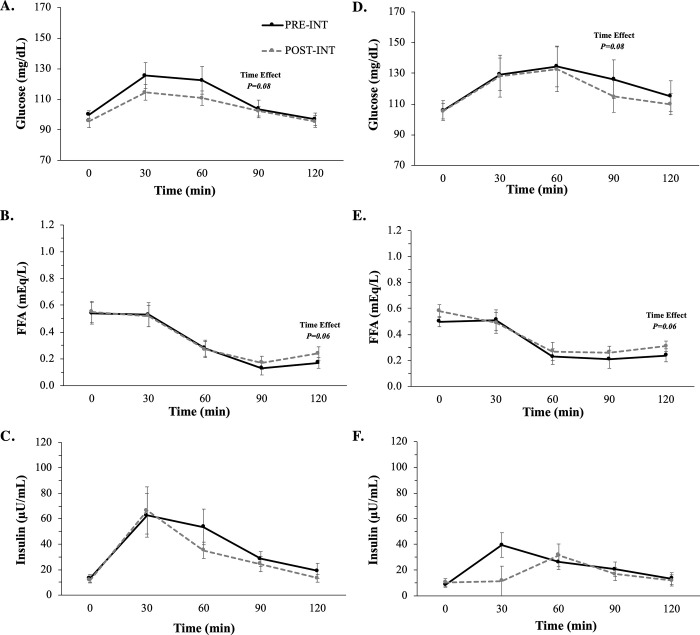
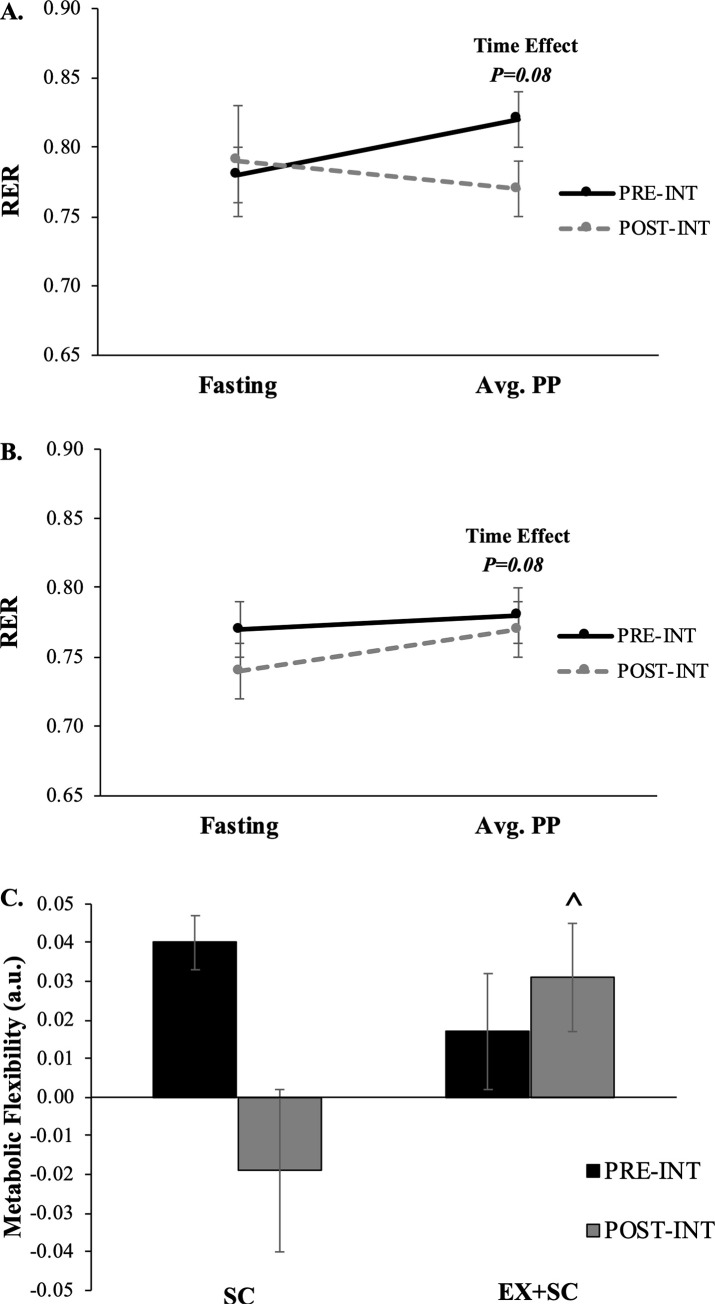
Methods: Fourteen bariatric patients (age: 42.3±2.5y, BMI: 45.1±2.5 kg/m2) met inclusion criteria and were match-paired to pre-operative SC (n = 7) or EX+SC (n = 7; walking 30min/d, 5d/wk, 65-85% HRpeak) for 30d. A 120min mixed meal tolerance test was performed pre- and post-intervention (~2d prior to surgery) to assess insulin sensitivity (Matsuda Index) and metabolic flexibility (indirect calorimetry). Aerobic fitness (VO2peak), body composition (BodPod), and adipokines (adiponectin, leptin) were also measured. Omental adipose tissue was collected during surgery to quantify gene expression of adiponectin and leptin, and operating time and length of hospital stay were recorded. ANOVA and Cohen's d effect size (ES) was used to test group differences.
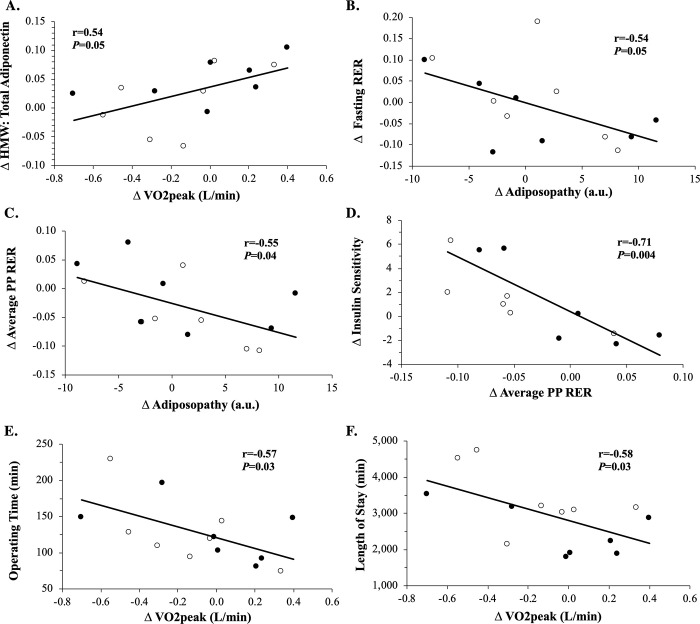
Results: SC tended to increase percent body fat (P = 0.06) after the intervention compared to EX+SC. Although SC and EX+SC tended to raise insulin sensitivity (P = 0.11), EX+SC enhanced metabolic flexibility (P = 0.01, ES = 1.55), reduced total adiponectin (P = 0.01, ES = 1.54) with no change in HMW adiponectin and decreased the length of hospital stay (P = 0.05) compared to SC. Albeit not statistically significant, EX+SC increased VO2peak 2.9% compared to a 5.9% decrease with SC (P = 0.24, ES = 0.91). This increased fitness correlated to shorter operating time (r = -0.57, P = 0.03) and length of stay (r = -0.58, P = 0.03). Less omental total adiponectin (r = 0.52, P = 0.09) and leptin (r = 0.58, P = 0.05) expression correlated with shorter operating time, and low leptin expression was linked to shorter length of stay (r = 0.70, P = 0.01), and low leptin expression was linked to shorter length of stay (r = 0.70, P = 0.01).
Conclusion: Adding pre-operative aerobic exercise to standard care may improve surgical outcomes through a fitness and adipose tissue derived mechanism.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Impact of Pre-operative Aerobic Exercise on Cardiometabolic Health and Quality of Life in Patients Undergoing Bariatric Surgery.Front Physiol. 2020 Aug 26;11:1018. doi: 10.3389/fphys.2020.01018. eCollection 2020. Front Physiol. 2020. PMID: 32982777 Free PMC article.
-
Effect of presurgical aerobic exercise on cardiometabolic health 30 days after bariatric surgery.Physiol Rep. 2021 Nov;9(21):e15039. doi: 10.14814/phy2.15039. Physiol Rep. 2021. PMID: 34713979 Free PMC article. Clinical Trial.
-
Urinary albumin excretion, HMW adiponectin, and insulin sensitivity in type 2 diabetic patients undergoing bariatric surgery.Obes Surg. 2010 Mar;20(3):308-15. doi: 10.1007/s11695-009-0026-1. Obes Surg. 2010. PMID: 20217955 Free PMC article.
-
Evaluation of the Effect of the Pre-Operative Exercise Training on Weight Loss, Quality of Life, and Cardiopulmonary Parameter in Bariatric Metabolic Surgery: A Systematic Review and Meta-Analysis.Obes Surg. 2024 Jul;34(7):2670-2684. doi: 10.1007/s11695-024-07333-y. Epub 2024 Jun 10. Obes Surg. 2024. PMID: 38856886
-
Towards Optimized Care After Bariatric Surgery by Physical Activity and Exercise Intervention: a Review.Obes Surg. 2020 Mar;30(3):1118-1125. doi: 10.1007/s11695-020-04390-x. Obes Surg. 2020. PMID: 31912467 Review.
Cited by
-
Acceptability and Feasibility of the Telehealth Bariatric Behavioral Intervention to Increase Physical Activity: Protocol for a Single-Case Experimental Study.JMIR Res Protoc. 2022 Sep 29;11(9):e39633. doi: 10.2196/39633. JMIR Res Protoc. 2022. PMID: 36173668 Free PMC article.
-
The Degree of Preoperative Hypoalbuminemia Is Associated with Risk of Postoperative Complications in Metabolic and Bariatric Surgery Patients.Obes Surg. 2024 Jan;34(1):51-70. doi: 10.1007/s11695-023-06944-1. Epub 2023 Nov 23. Obes Surg. 2024. PMID: 37994997
-
Preoperative Physical Activity Level and Exercise Prescription in Adults With Obesity: The Effect on Post-Bariatric Surgery Outcomes.Front Physiol. 2022 Jul 6;13:869998. doi: 10.3389/fphys.2022.869998. eCollection 2022. Front Physiol. 2022. PMID: 35874538 Free PMC article.
-
Effect of exercise training before and after bariatric surgery: A systematic review and meta-analysis.Obes Rev. 2021 Jul;22 Suppl 4(Suppl 4):e13296. doi: 10.1111/obr.13296. Epub 2021 Jun 3. Obes Rev. 2021. PMID: 34080281 Free PMC article.
-
Impact of Pre-operative Aerobic Exercise on Cardiometabolic Health and Quality of Life in Patients Undergoing Bariatric Surgery.Front Physiol. 2020 Aug 26;11:1018. doi: 10.3389/fphys.2020.01018. eCollection 2020. Front Physiol. 2020. PMID: 32982777 Free PMC article.
References
-
- Li JF, Lai DD, Lin ZH, Jiang TY, Zhang AM, Dai JF. Comparison of the long-term results of Roux-en-Y gastric bypass and sleeve gastrectomy for morbid obesity: a systematic review and meta-analysis of randomized and nonrandomized trials. Surg Laparosc Endosc Percutan Tech. 2014;24: 1–11. 10.1097/SLE.0000000000000041 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
