

Do assets explain the relation between race/ethnicity and probable depression in U.S. adults?
- PMID: 33006988
- PMCID: PMC7531850
- DOI: 10.1371/journal.pone.0239618
Do assets explain the relation between race/ethnicity and probable depression in U.S. adults?
Abstract
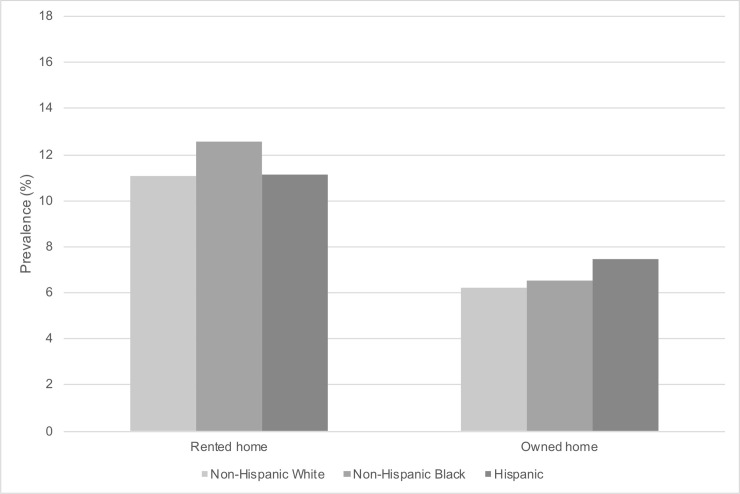
Depression is a leading cause of disability in the U.S. across all race/ethnicity groups. While non-Hispanic Black and Hispanic persons have worse physical health on most indicators than non-Hispanic White persons, the literature on the association between race/ethnicity and rates of depression is mixed. Given unequal distribution of assets across racial/ethnic groups, it is possible that social and economic differences may explain differential rates of depression across race/ethnicity groups. Using National Health and Nutrition Examination Survey (NHANES) data from 2007-2016, we constructed a nationally representative sample of 26,382 adults over 18 years old (11,072 non-Hispanic White, 5,610 non-Hispanic Black, 6,981 Hispanic, and 2,719 Other race). We measured symptoms of depression using the Patient Health Questionnaire-9 (PHQ-9), with a score of 10 or more indicating probable depression. We identified three kinds of assets: financial assets (income), physical assets (home ownership), and social assets (marital status and education). We estimated the weighted prevalence of probable depression across race/ethnicity groups, odds ratios controlling for assets, and predicted probabilities of probable depression across race/ethnicity and asset groups. Three results contribute to our understanding of the differences in probable depression rates between race/ethnicity groups: 1) Non-Hispanic Black and Hispanic persons had a higher weighted prevalence of probable depression in the U.S. than non-Hispanic White persons. In models unadjusted for assets, non-Hispanic Black and Hispanic persons had 1.3 greater odds of probable depression than non-Hispanic White persons (p<0.01). 2) We found an inverse relation between assets and probable depression across all race-ethnicity groups. Also, non-Hispanic Black and Hispanic persons had fewer assets than non-Hispanic Whites. 3) When we controlled for assets, non-Hispanic Black and Hispanic persons had 0.8 times lower odds of probable depression than non-Hispanic White persons (p<0.05). Thus, when holding assets constant, minorities had better mental health than non-Hispanic White persons in the U.S. These three findings help to reconcile findings in the literature on race/ethnicity and depression. Given vastly unequal distribution of wealth in the U.S., it is not surprising that racial minorities, who hold fewer assets, would have an overall larger prevalence of mental illness, as seen in unadjusted estimates. Once assets are taken into account, Black and Hispanic persons appear to have better mental health than non-Hispanic White persons. Assets may explain much of the relation between race/ethnicity group and depression in the U.S. Future research should consider the role of assets in protecting against mental illness.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Building Financial Capability and Assets to Reduce Poverty and Health Disparities: Race/Ethnicity Matters.J Racial Ethn Health Disparities. 2024 Jun;11(3):1754-1773. doi: 10.1007/s40615-023-01648-9. Epub 2023 Jun 5. J Racial Ethn Health Disparities. 2024. PMID: 37273162
-
Racial, Ethnic, and Socioeconomic Differences in Food Allergies in the US.JAMA Netw Open. 2023 Jun 1;6(6):e2318162. doi: 10.1001/jamanetworkopen.2023.18162. JAMA Netw Open. 2023. PMID: 37314805 Free PMC article.
-
Racial and ethnic differences in perception of provider cultural competence among patients with depression and anxiety symptoms: a retrospective, population-based, cross-sectional analysis.Lancet Psychiatry. 2021 Nov;8(11):957-968. doi: 10.1016/S2215-0366(21)00285-6. Epub 2021 Sep 23. Lancet Psychiatry. 2021. PMID: 34563316 Free PMC article.
-
Comparing Preferences for Depression and Diabetes Treatment among Adults of Different Racial and Ethnic Groups Who Reported Discrimination in Health Care [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jan. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jan. PMID: 38478703 Free Books & Documents. Review.
-
Sociodemographic Characteristics of Persons With Diabetes.In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 8. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 8. PMID: 33651553 Free Books & Documents. Review.
Cited by
-
Racial Differences in Head Pain and Other Pain-Related Outcomes After Mild Traumatic Brain Injury.J Neurotrauma. 2023 Aug;40(15-16):1671-1683. doi: 10.1089/neu.2022.0415. Epub 2023 Feb 24. J Neurotrauma. 2023. PMID: 36565020 Free PMC article.
-
Area-level credit scores and symptoms of depression and anxiety in adults.Am J Epidemiol. 2025 May 7;194(5):1208-1220. doi: 10.1093/aje/kwae275. Am J Epidemiol. 2025. PMID: 39160639 Free PMC article.
-
Prevalence estimates of depression and anxiety symptoms among adolescents in Bermuda, according to age, gender and race.Soc Psychiatry Psychiatr Epidemiol. 2025 Sep;60(9):2189-2200. doi: 10.1007/s00127-025-02829-z. Epub 2025 Mar 11. Soc Psychiatry Psychiatr Epidemiol. 2025. PMID: 40067365 Free PMC article.
-
URMC Universal Depression Screening Initiative: Patient Reported Outcome Assessments to Promote a Person-Centered Biopsychosocial Population Health Management Strategy.Front Psychiatry. 2022 Jan 11;12:796499. doi: 10.3389/fpsyt.2021.796499. eCollection 2021. Front Psychiatry. 2022. PMID: 35087432 Free PMC article.
-
Sleep Apnea and Substance Use Disorders Associated with Co-Occurrence of Anxiety Disorder and Depression among U.S. Adults: Findings from the NSDUH 2008-2014.Brain Sci. 2023 Apr 14;13(4):661. doi: 10.3390/brainsci13040661. Brain Sci. 2023. PMID: 37190626 Free PMC article.
References
-
- Brody D, Pratt L, Hughes J. Prevalence of depression among adults aged 20 and over: United States, 2013–2016 [Internet]. U.S. Department of Health and Human Services Centers for Disease Control and Prevention National Center for Health Statistics; 2018 Feb. Report No.: 303. Available from: https://www.cdc.gov/nchs/products/databriefs/db303.htm
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
