

Evaluation of a digital triage platform in Uganda: A quality improvement initiative to reduce the time to antibiotic administration
- PMID: 33007047
- PMCID: PMC7531789
- DOI: 10.1371/journal.pone.0240092
Evaluation of a digital triage platform in Uganda: A quality improvement initiative to reduce the time to antibiotic administration
Abstract
Background: Sepsis is the leading cause of death in children under five in low- and middle-income countries. The rapid identification of the sickest children and timely antibiotic administration may improve outcomes. We developed and implemented a digital triage platform to rapidly identify critically ill children to facilitate timely intravenous antibiotic administration.
Objective: This quality improvement initiative sought to reduce the time to antibiotic administration at a dedicated children's hospital outpatient department in Mbarara, Uganda.
Intervention and study design: The digital platform consisted of a mobile application that collects clinical signs, symptoms, and vital signs to prioritize children through a combination of emergency triggers and predictive risk algorithms. A computer-based dashboard enabled the prioritization of children by displaying an overview of all children and their triage categories. We evaluated the impact of the digital triage platform over an 11-week pre-implementation phase and an 11-week post-implementation phase. The time from the end of triage to antibiotic administration was compared to evaluate the quality improvement initiative.
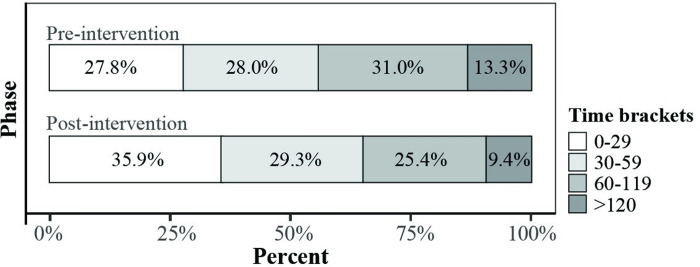
Results: There was a difference of -11 minutes (95% CI, -16.0 to -6.0; p < 0.001; Mann-Whitney U test) in time to antibiotics, from 51 minutes (IQR, 27.0-94.0) pre-implementation to 44 minutes (IQR, 19.0-74.0) post-implementation. Children prioritized as emergency received the greatest time benefit (-34 minutes; 95% CI, -9.0 to -58.0; p < 0.001; Mann-Whitney U test). The proportion of children who waited more than an hour until antibiotics decreased by 21.4% (p = 0.007).
Conclusion: A data-driven patient prioritization and continuous feedback for healthcare workers enabled by a digital triage platform led to expedited antibiotic therapy for critically ill children with sepsis. This platform may have a more significant impact in facilities without existing triage processes and prioritization of treatments, as is commonly encountered in low resource settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- The UN Inter-Agency Group for Child Mortality Estimation. Levels and trends in child mortality: report 2019. New York: UNICEF; 2019. Available from: https://childmortality.org/wp-content/uploads/2019/09/UN-IGME-Child-Mort...
-
- United Nations. Transforming our world: The 2030 agenda for sustainable development. 2015. New York, United States: United Nations; 2015. Available from: https://sustainabledevelopment.un.org/post2015/transformingourworld/publ...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
