

The association of smoking status with SARS-CoV-2 infection, hospitalization and mortality from COVID-19: a living rapid evidence review with Bayesian meta-analyses (version 7)
- PMID: 33007104
- PMCID: PMC7590402
- DOI: 10.1111/add.15276
The association of smoking status with SARS-CoV-2 infection, hospitalization and mortality from COVID-19: a living rapid evidence review with Bayesian meta-analyses (version 7)
Abstract
Aims: To estimate the association of smoking status with rates of (i) infection, (ii) hospitalization, (iii) disease severity and (iv) mortality from SARS-CoV-2/COVID-19 disease.
Design: Living rapid review of observational and experimental studies with random-effects hierarchical Bayesian meta-analyses. Published articles and pre-prints were identified via MEDLINE and medRxiv.
Setting: Community or hospital, no restrictions on location.
Participants: Adults who received a SARS-CoV-2 test or a COVID-19 diagnosis.
Measurements: Outcomes were SARS-CoV-2 infection, hospitalization, disease severity and mortality stratified by smoking status. Study quality was assessed (i.e. 'good', 'fair' and 'poor').
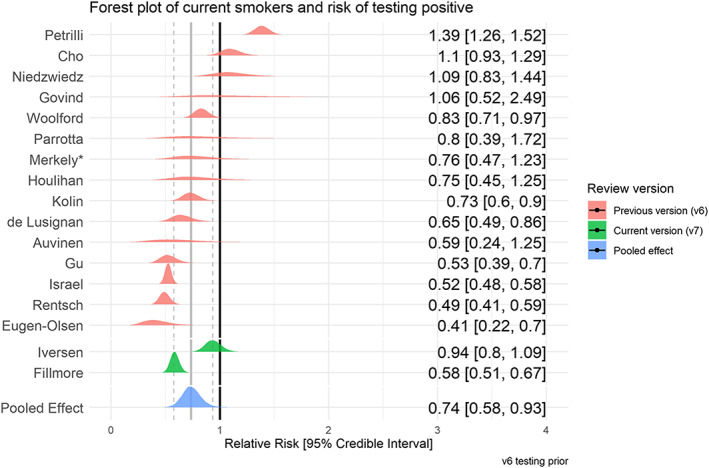
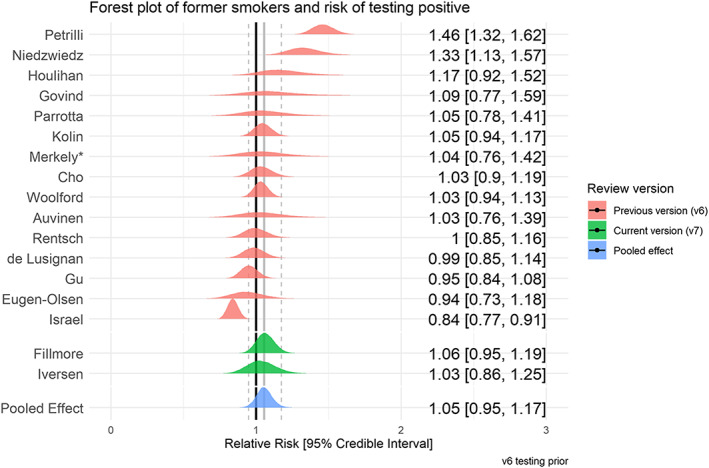
Findings: Version 7 (searches up to 25 August 2020) included 233 studies with 32 'good' and 'fair' quality studies included in meta-analyses. Fifty-seven studies (24.5%) reported current, former and never smoking status. Recorded smoking prevalence among people with COVID-19 was generally lower than national prevalence. Current compared with never smokers were at reduced risk of SARS-CoV-2 infection [relative risk (RR) = 0.74, 95% credible interval (CrI) = 0.58-0.93, τ = 0.41]. Data for former smokers were inconclusive (RR = 1.05, 95% CrI = 0.95-1.17, τ = 0.17), but favoured there being no important association (21% probability of RR ≥ 1.1). Former compared with never smokers were at somewhat increased risk of hospitalization (RR = 1.20, CrI = 1.03-1.44, τ = 0.17), greater disease severity (RR = 1.52, CrI = 1.13-2.07, τ = 0.29) and mortality (RR = 1.39, 95% CrI = 1.09-1.87, τ = 0.27). Data for current smokers were inconclusive (RR = 1.06, CrI = 0.82-1.35, τ = 0.27; RR = 1.25, CrI = 0.85-1.93, τ = 0.34; RR = 1.22, 95% CrI = 0.78-1.94, τ = 0.49, respectively), but favoured there being no important associations with hospitalization and mortality (35% and 70% probability of RR ≥ 1.1, respectively) and a small but important association with disease severity (79% probability of RR ≥ 1.1).
Conclusions: Compared with never smokers, current smokers appear to be at reduced risk of SARS-CoV-2 infection, while former smokers appear to be at increased risk of hospitalization, increased disease severity and mortality from COVID-19. However, it is uncertain whether these associations are causal.
Keywords: COVID-19; SARS-CoV-2; e-cigarettes; hospitalization; infection; living review; mortality; nicotine replacement therapy; smoking; tobacco.
© 2020 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures









Comment in
-
Commentary on Simons et al. Public health implications of the suggested association between nicotine, smoking and infection with SARS-CoV-2.Addiction. 2021 Jun;116(6):1369-1370. doi: 10.1111/add.15356. Epub 2020 Dec 25. Addiction. 2021. PMID: 33368844 No abstract available.
References
-
- Cai G. Bulk and single‐cell transcriptomics identify tobacco‐use disparity in lung gene expression of ACE2, the receptor of 2019‐nCov. medRxiv 2020; 10.20944/preprints202002.0051.v3 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
