

Contribution of Individual and Neighborhood Factors to Racial Disparities in Respiratory Outcomes
- PMID: 33007162
- PMCID: PMC8048743
- DOI: 10.1164/rccm.202002-0253OC
Contribution of Individual and Neighborhood Factors to Racial Disparities in Respiratory Outcomes
Abstract
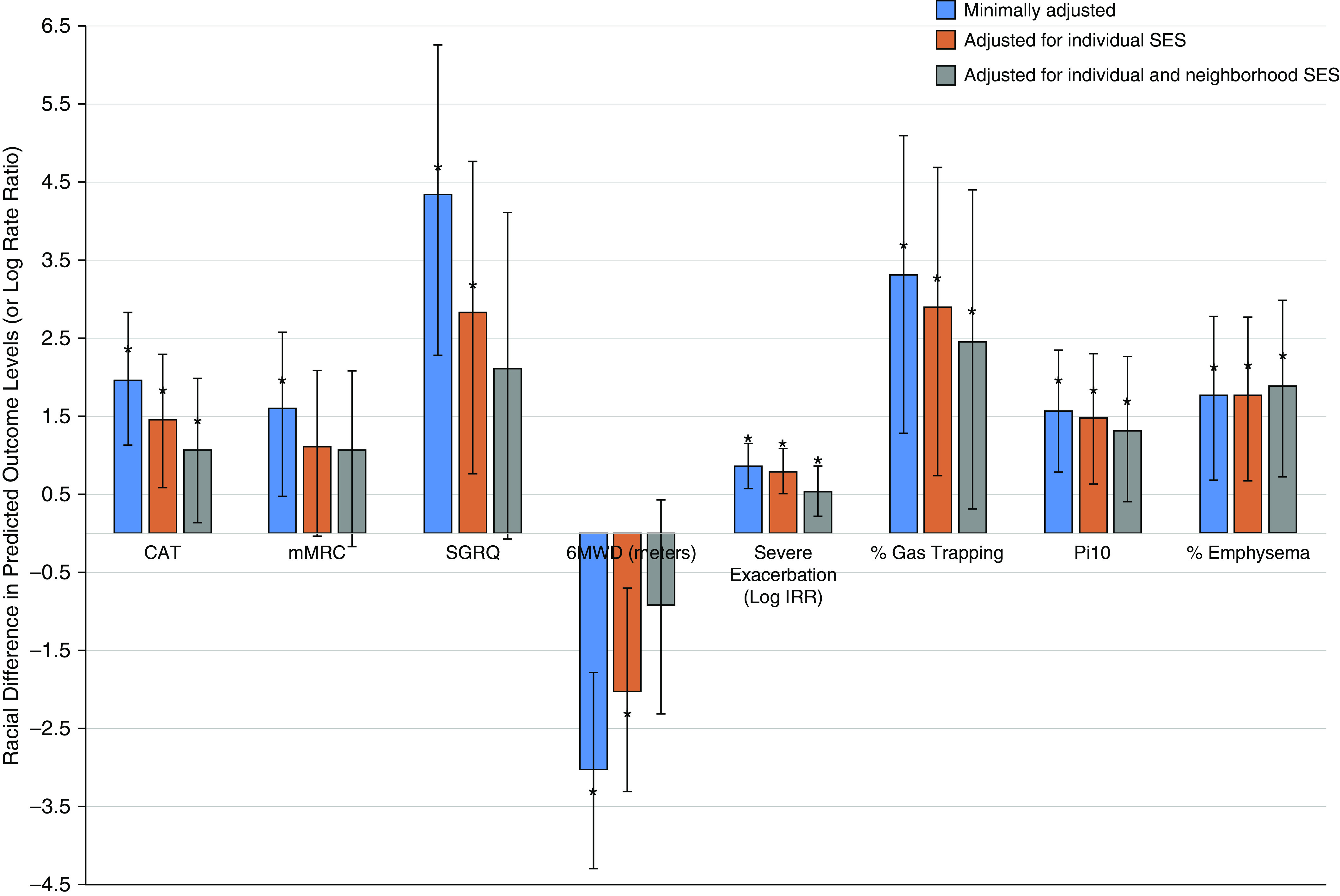
Rationale: Black adults have worse health outcomes compared with white adults in certain chronic diseases, including chronic obstructive pulmonary disease (COPD).Objectives: To determine to what degree disadvantage by individual and neighborhood socioeconomic status (SES) may contribute to racial disparities in COPD outcomes.Methods: Individual and neighborhood-scale sociodemographic characteristics were determined in 2,649 current or former adult smokers with and without COPD at recruitment into SPIROMICS (Subpopulations and Intermediate Outcome Measures in COPD Study). We assessed whether racial differences in symptom, functional, and imaging outcomes (St. George's Respiratory Questionnaire, COPD Assessment Test score, modified Medical Research Council dyspnea scale, 6-minute-walk test distance, and computed tomography [CT] scan metrics) and severe exacerbation risk were explained by individual or neighborhood SES. Using generalized linear mixed model regression, we compared respiratory outcomes by race, adjusting for confounders and individual-level and neighborhood-level descriptors of SES both separately and sequentially.Measurements and Main Results: After adjusting for COPD risk factors, Black participants had significantly worse respiratory symptoms and quality of life (modified Medical Research Council scale, COPD Assessment Test, and St. George's Respiratory Questionnaire), higher risk of severe exacerbations and higher percentage of emphysema, thicker airways (internal perimeter of 10 mm), and more air trapping on CT metrics compared with white participants. In addition, the association between Black race and respiratory outcomes was attenuated but remained statistically significant after adjusting for individual-level SES, which explained up to 12-35% of racial disparities. Further adjustment showed that neighborhood-level SES explained another 26-54% of the racial disparities in respiratory outcomes. Even after accounting for both individual and neighborhood SES factors, Black individuals continued to have increased severe exacerbation risk and persistently worse CT outcomes (emphysema, air trapping, and airway wall thickness).Conclusions: Disadvantages by individual- and neighborhood-level SES each partly explain disparities in respiratory outcomes between Black individuals and white individuals. Strategies to narrow the gap in SES disadvantages may help to reduce race-related health disparities in COPD; however, further work is needed to identify additional risk factors contributing to persistent disparities.
Keywords: COPD; neighborhood disadvantage; racial disparities; socioeconomic status.
Figures
Comment in
-
The Role of Individual and Neighborhood Factors on Racial Disparity in Respiratory Outcomes. Won't You Be My Neighbor?Am J Respir Crit Care Med. 2021 Apr 15;203(8):939-940. doi: 10.1164/rccm.202010-3875ED. Am J Respir Crit Care Med. 2021. PMID: 33296282 Free PMC article. No abstract available.
References
-
- Kelly RL. Age adjusted to 2000 standard population: all ages. Per 100,000 population. 2015 Kelly Report: health disparities in America. 2015 [accessed 2019 Apr 16]. Available from: https://robinkelly.house.gov/sites/robinkelly.house.gov/files/2015%20Kel....
-
- Sarrazin MV, Cannon KT, Rosenthal GE, Kaldjian LC. Racial differences in mortality among veterans hospitalized for exacerbation of chronic obstructive pulmonary disease. J Natl Med Assoc. 2009;101:656–662. - PubMed
-
- Prescott E, Godtfredsen N, Vestbo J, Osler M. Social position and mortality from respiratory diseases in males and females. Eur Respir J. 2003;21:821–826. - PubMed
Publication types
MeSH terms
Grants and funding
- P50 MD010431/MD/NIMHD NIH HHS/United States
- HHSN268200900019C/HL/NHLBI NIH HHS/United States
- K23 ES025781/ES/NIEHS NIH HHS/United States
- R01 ES023500/ES/NIEHS NIH HHS/United States
- HHSN268200900015C/HL/NHLBI NIH HHS/United States
- HHSN268200900016C/HL/NHLBI NIH HHS/United States
- P30 ES007033/ES/NIEHS NIH HHS/United States
- U01 HL137880/HL/NHLBI NIH HHS/United States
- K23 HL153672/HL/NHLBI NIH HHS/United States
- HHSN268200900018C/HL/NHLBI NIH HHS/United States
- HHSN268200900013C/HL/NHLBI NIH HHS/United States
- HHSN268200900014C/HL/NHLBI NIH HHS/United States
- K24 HL138188/HL/NHLBI NIH HHS/United States
- T32 HL007534/HL/NHLBI NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- K23 HL123778/HL/NHLBI NIH HHS/United States
- K24 HL137013/HL/NHLBI NIH HHS/United States
- HHSN268200900017C/HL/NHLBI NIH HHS/United States
- HHSN268200900020C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
