

Management of clinical chorioamnionitis: an evidence-based approach
- PMID: 33007269
- PMCID: PMC8315154
- DOI: 10.1016/j.ajog.2020.09.044
Management of clinical chorioamnionitis: an evidence-based approach
Abstract
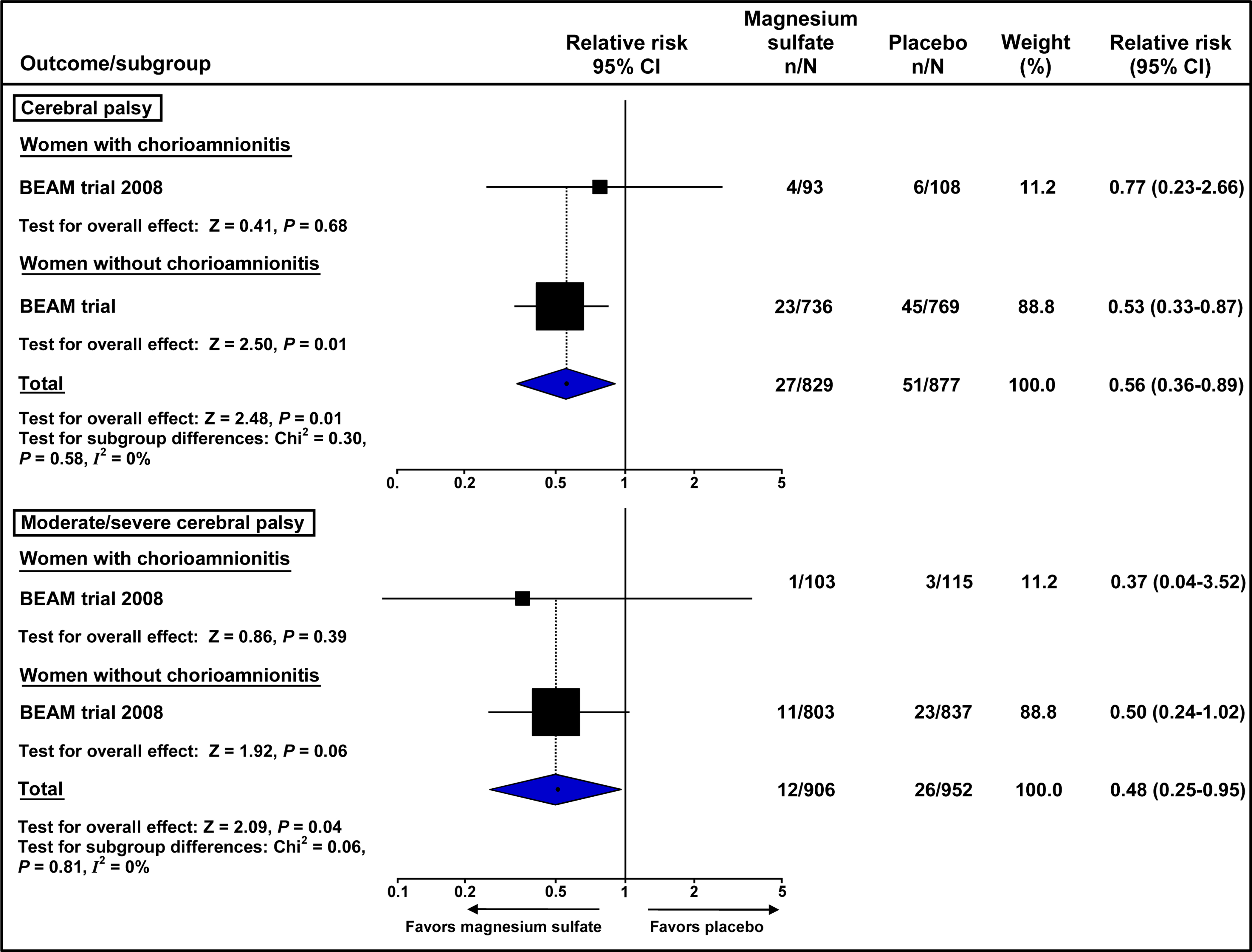
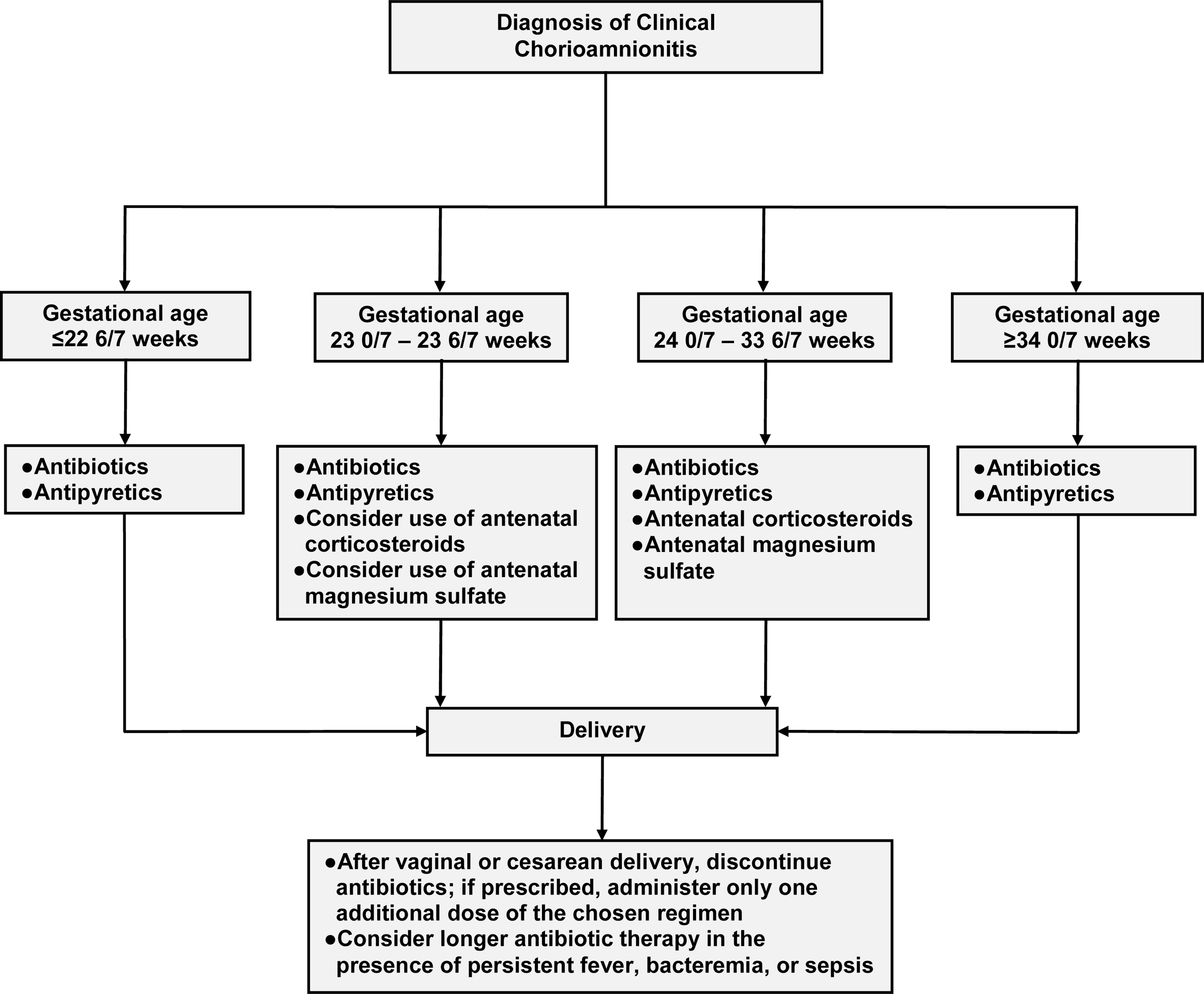
This review aimed to examine the existing evidence about interventions proposed for the treatment of clinical chorioamnionitis, with the goal of developing an evidence-based contemporary approach for the management of this condition. Most trials that assessed the use of antibiotics in clinical chorioamnionitis included patients with a gestational age of ≥34 weeks and in labor. The first-line antimicrobial regimen for the treatment of clinical chorioamnionitis is ampicillin combined with gentamicin, which should be initiated during the intrapartum period. In the event of a cesarean delivery, patients should receive clindamycin at the time of umbilical cord clamping. The administration of additional antibiotic therapy does not appear to be necessary after vaginal or cesarean delivery. However, if postdelivery antibiotics are prescribed, there is support for the administration of an additional dose. Patients can receive antipyretic agents, mainly acetaminophen, even though there is no clear evidence of their benefits. Current evidence suggests that the administration of antenatal corticosteroids for fetal lung maturation and of magnesium sulfate for fetal neuroprotection to patients with clinical chorioamnionitis between 24 0/7 and 33 6/7 weeks of gestation, and possibly between 23 0/7 and 23 6/7 weeks of gestation, has an overall beneficial effect on the infant. However, delivery should not be delayed to complete the full course of corticosteroids and magnesium sulfate. Once the diagnosis of clinical chorioamnionitis has been established, delivery should be considered, regardless of the gestational age. Vaginal delivery is the safer option and cesarean delivery should be reserved for standard obstetrical indications. The time interval between the diagnosis of clinical chorioamnionitis and delivery is not related to most adverse maternal and neonatal outcomes. Patients may require a higher dose of oxytocin to achieve adequate uterine activity or greater uterine activity to effect a given change in cervical dilation. The benefit of using continuous electronic fetal heart rate monitoring in these patients is unclear. We identified the following promising interventions for the management of clinical chorioamnionitis: (1) an antibiotic regimen including ceftriaxone, clarithromycin, and metronidazole that provides coverage against the most commonly identified microorganisms in patients with clinical chorioamnionitis; (2) vaginal cleansing with antiseptic solutions before cesarean delivery with the aim of decreasing the risk of endometritis and, possibly, postoperative wound infection; and (3) antenatal administration of N-acetylcysteine, an antioxidant and antiinflammatory agent, to reduce neonatal morbidity and mortality. Well-powered randomized controlled trials are needed to assess these interventions in patients with clinical chorioamnionitis.
Keywords: N-acetylcysteine; abnormal fetal heart rate patterns; abnormal labor progression; adverse maternal outcomes; adverse neonatal outcomes; antenatal corticosteroids; antibiotics; antipyretic agents; cerebral palsy; cesarean delivery; continuous electronic fetal heart rate monitoring; fever; intraamniotic infection; intraamniotic inflammation; magnesium sulfate; management of labor; maternal infection; neonatal sepsis; neuroprotection; postpartum hemorrhage; prolonged labor; vaginal cleansing.
Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Malloy MH. Chorioamnionitis: epidemiology of newborn management and outcome United States 2008. J Perinatol 2014;34:611–5. - PubMed
-
- Braun D, Bromberger P, Ho NJ, Getahun D. Low rate of perinatal sepsis in term Infants of mothers with chorioamnionitis. Am J Perinatol 2016;33:143–50. - PubMed
-
- Perry AK, Rossi RM, DeFranco EA. Severe adverse maternal outcomes associated with chorioamnionitis. Am J Obstet Gynecol MFM 2019;1:100027. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
