

Learning curves in atrial fibrillation ablation - A comparison between second generation cryoballoon and contact force sensing radiofrequency catheters
- PMID: 33007406
- PMCID: PMC7691769
- DOI: 10.1016/j.ipej.2020.09.003
Learning curves in atrial fibrillation ablation - A comparison between second generation cryoballoon and contact force sensing radiofrequency catheters
Abstract
Objective: To examine the learning curves of atrial fibrillation (AF) ablation comparing the cryoballoon (CB) and radiofrequency (RF) catheters.
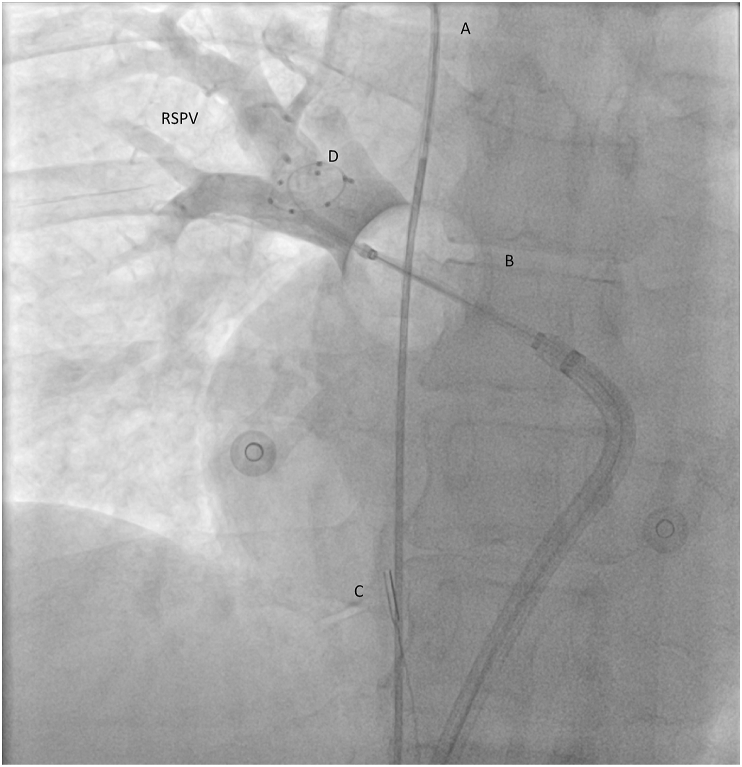
Methods: We performed a retrospective data analysis from the initiation of AF ablation program in our center. For CB ablation, a second generation 28 mm balloon was utilized and for RF ablation.
Results: A total of 100 consecutive patients (50 in each group) have been enrolled in the study (male 74%, mean age 58.9 ± 10 years, paroxysmal AF 85%). The mean procedure time was shorter for CB (116.6 ± 39.8 min) than RF group (191.8 ± 101.1 min) (p < 0.001). There was no difference in the mean fluoroscopy time, 24.2 ± 10.6 min in RF and 22.4 ± 11.7 min in CB group, (p = 0.422). Seven major complications occurred during the study; 5 in RF group (10%) and 2 in CB group (4%) (p = 0.436). After the mean follow up of 14.5 ± 2.4 months, 15 patients in RF group (30%) and 11 in CB group (26%) experienced AF recurrences (P = 0.300).
Conclusion: When starting a new AF ablation program, our results suggest that CB significantly shortens procedure while fluoroscopy time and clinical outcomes are comparable to RF ablation.
Keywords: Ablation; Atrial fibrillation; Contact force sensing radiofrequency catheters; Second generation cryoballoon.
Copyright © 2020 Indian Heart Rhythm Society. Production and hosting by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest Conflict of interest: VV received an educational grants by St Jude Medical, travel grants and lecture fees from Medtronic and Biosense-Webster. MP received educational and travel grants from Medtronic and Biosense-Webster. Conflict of interest: VV received an educational grants by St Jude Medical, travel grants and lecture fees from Medtronic and Biosense-Webster. MP received educational and travel grants from Medtronic and Biosense-Webster.
Figures





References
-
- Haim M., Hoshen M., Reges O., Rabi Y., Balicer R., Leibowitz M. Prospective national study of the prevalence, incidence, management and outcome of a large contemporary cohort of patients with incident non-valvular atrial fibrillation. J Am Heart Assoc. 2015;4 doi: 10.1161/JAHA.114.001486. - DOI - PMC - PubMed
-
- Krijthe B.P., Kunst A., Benjamin E.J., Lip G.Y., Franco O.H., Hofman A., Witteman J.C., Stricker B.H., Heeringa J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. 2013;34:2746–2751. doi: 10.1093/eurheartj/eht280. - DOI - PMC - PubMed
-
- Calkins H., Kuck K.H., Cappato R. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012;14:528–606. doi: 10.1093/europace/eus027. 2012. - DOI - PubMed
-
- Arbelo E., Brugada J., Hindricks G. Atrial fibrillation ablation pilot study investigators: ESCEURObservational research programme: the atrial fibrillation ablation pilot study, conducted by the European heart rhythm association. Europace. 2012;14:1094–1103. doi: 10.1093/europace/eus153. - DOI - PubMed
LinkOut - more resources
Full Text Sources
