

Rationale and Design of the Future Optimal Research and Care Evaluation in Patients with Acute Coronary Syndrome (FORCE-ACS) Registry: Towards "Personalized Medicine" in Daily Clinical Practice
- PMID: 33007932
- PMCID: PMC7601438
- DOI: 10.3390/jcm9103173
Rationale and Design of the Future Optimal Research and Care Evaluation in Patients with Acute Coronary Syndrome (FORCE-ACS) Registry: Towards "Personalized Medicine" in Daily Clinical Practice
Abstract
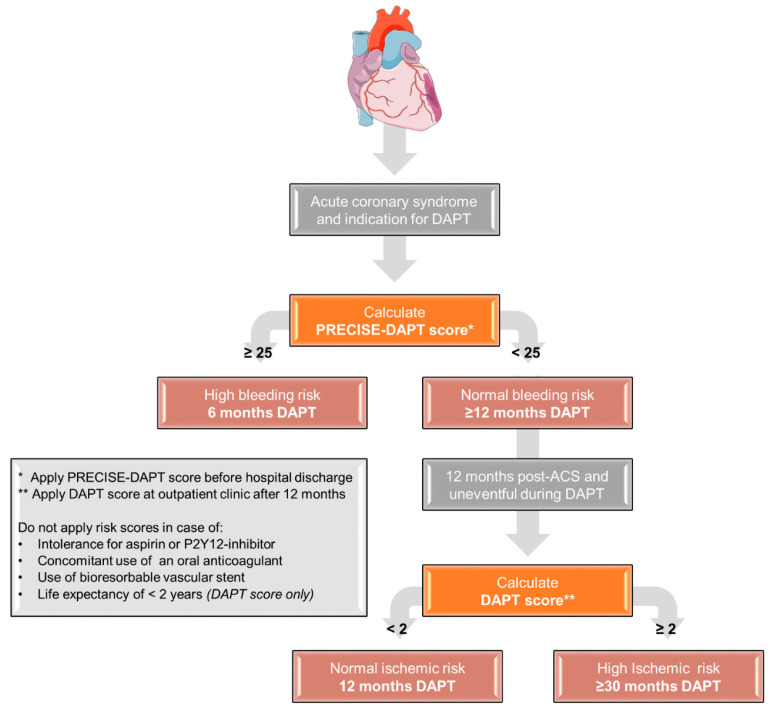
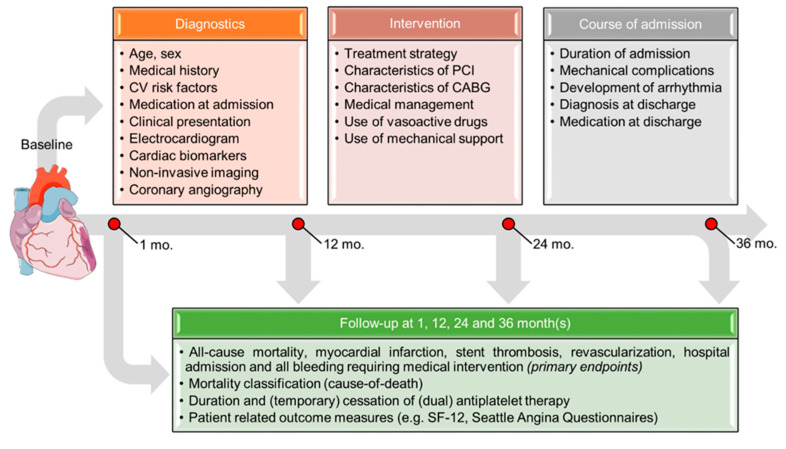
Diagnostic and treatment strategies for acute coronary syndrome have improved dramatically over the past few decades, but mortality and recurrent myocardial infarction rates remain high. An aging population with increasing co-morbidities heralds new clinical challenges. Therefore, in order to evaluate and improve current treatment strategies, detailed information on clinical presentation, treatment and follow-up in real-world patients is needed. The Future Optimal Research and Care Evaluation in patients with Acute Coronary Syndrome (FORCE-ACS) registry (ClinicalTrials.gov Identifier: NCT03823547) is a multi-center, prospective real-world registry of patients admitted with (suspected) acute coronary syndrome. Both non-interventional and interventional cardiac centers in different regions of the Netherlands are currently participating. Patients are treated according to local protocols, enabling the evaluation of different diagnostic and treatment strategies used in daily practice. Data collection is performed using electronic medical records and quality-of-life questionnaires, which are sent 1, 12, 24 and 36 months after initial admission. Major end points are all-cause mortality, myocardial infarction, stent thrombosis, stroke, revascularization and all bleeding requiring medical attention. Invasive therapy, antithrombotic therapy including patient-tailored strategies, such as the use of risk scores, pharmacogenetic guided antiplatelet therapy and patient reported outcome measures are monitored. The FORCE-ACS registry provides insight into numerous aspects of the (quality of) care for acute coronary syndrome patients.
Keywords: acute coronary syndrome; antiplatelet therapy; multicenter registry.
Conflict of interest statement
J.P.S.H. has received unrestricted grants from AstraZeneca; W.J.K. has received research grants and speaker fees from AstraZeneca; J.M.t.B. has received research grants from ZonMw and AstraZeneca and Advisory/consulting/speaker fees from AstraZeneca, Eli Lilly, Daiichi Sankyo, The Medicines Company, Accu-Meterics, Boehringer Ingelheim, BMS, Pfizer, Payer, Ferrer, Idorsia. D.R.P.P.C.P.Y., G.-J.A.V., N.M.R.v.d.S., R.W., R.M.T.J.G., D.M.N., J.L., D.M.F.C., M.E.G., J.A., W.L.B., T.O., J.D., G.J.V., R.J.v.B. and Y.A. declare to have no conflict of interest. The funders had no role in the design of the study or in the writing of the manuscript.
Figures

References
-
- Szummer K., Wallentin L., Lindhagen L., Alfredsson J., Erlinge D., Held C., James S., Kellerth T., Lindahl B., Ravn-Fischer A., et al. Improved outcomes in patients with ST-elevation myocardial infarction during the last 20 years are related to implementation of evidence-based treatments: Experiences from the SWEDEHEART registry 1995–2014. Eur. Heart J. 2017;38:3056–3065. doi: 10.1093/eurheartj/ehx515. - DOI - PMC - PubMed
-
- Szummer K., Wallentin L., Lindhagen L., Alfredsson J., Erlinge D., Held C., James S., Kellerth T., Lindahl B., Ravn-Fischer A., et al. Relations between implementation of new treatments and improved outcomes in patients with non-ST-elevation myocardial infarction during the last 20 years: Experiences from SWEDEHEART registry 1995 to 2014. Eur. Heart J. 2018;39:3766–3776. doi: 10.1093/eurheartj/ehy554. - DOI - PubMed
-
- Fox K.A.A., Carruthers K.F., Dunbar D.R., Graham C., Manning J.R., De Raedt H., Buysschaert I., Lambrechts D., Van De Werf F. Underestimated and under-recognized: The late consequences of acute coronary syndrome (GRACE UK-Belgian Study) Eur. Heart J. 2010;31:2755–2764. doi: 10.1093/eurheartj/ehq326. - DOI - PubMed
-
- Simonsson M., Wallentin L., Alfredsson J., Erlinge D., Hellstrom Angerud K., Hofmann R., Kellerth T., Lindhagen L., Ravn-Fischer A., Szummer K., et al. Temporal trends in bleeding events in acute myocardial infarction: Insights from the SWEDEHEART registry. Eur. Heart J. 2020;41:833–843. doi: 10.1093/eurheartj/ehz593. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
