

Innovative rehabilitative bracing with applied resistance improves walking pattern recovery in the early stages of rehabilitation after ACL reconstruction: a preliminary investigation
- PMID: 33008346
- PMCID: PMC7532107
- DOI: 10.1186/s12891-020-03661-z
Innovative rehabilitative bracing with applied resistance improves walking pattern recovery in the early stages of rehabilitation after ACL reconstruction: a preliminary investigation
Abstract
Background: The use of knee braces early after anterior cruciate ligament (ACL) reconstruction is a controversial issue. The study preliminarily compares the effect of a traditional brace blocked in knee extension and a new functional brace equipped with a spring resistance on walking and strength performance early after ACL reconstruction performed in the acute/subacute stage.
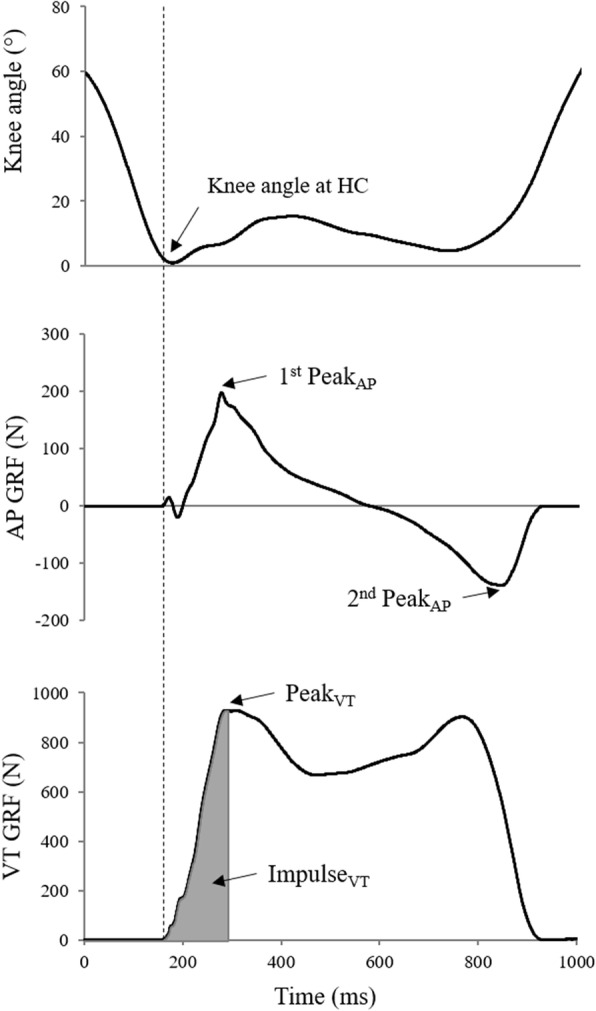
Methods: 14 ACL-reconstructed patients wore either a traditional (Control group: CG, 7 subjects) or a new functional brace (Experimental group: EG 7 subjects) until the 30th post-operative day. All patients were tested before surgery (T0), 15, 30, and 60 days after surgery (T1, T2, and T3, respectively). Knee angular displacement and ground reaction forces (GRF) during the stance phase of the gait cycle were analyzed at each session and, at T3, maximal voluntary isometric contraction (MVIC) for knee flexor/extensor muscles was performed. Limb symmetry indexes (LSI) of GRF and MVIC parameters were calculated.
Results: At T3, EG showed greater peak knee flexion angle of injured limb compared to CG (41 ± 2° vs 32 ± 1°, p < 0.001). During weight acceptance, a significant increase of anteroposterior GRF peak and vertical impulse from T1 to T3 was observed in the injured limb in EG (p < 0.05) but not in CG (p > 0.05). EG showed a greater side-to-side LSI of weight acceptance peak of anteroposterior GRF at T2 (113 ± 23% vs 69 ± 11%, p < 0.05) and T3 (112 ± 23% vs 84 ± 10%, p < 0.05).
Conclusions: The preliminary findings from this study indicate that the new functional brace did help in improving gait biomechanical pattern in the first two months after ACL reconstruction compared to a traditional brace locked in knee extension.
Keywords: Anterior cruciate ligament; Biomechanics; Brace; Gait; Rehabilitation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Effect of knee extension constraint training on walking biomechanics 6 months after anterior cruciate ligament reconstruction: a double-blind randomized controlled clinical trial.J Orthop Surg Res. 2025 Jan 7;20(1):20. doi: 10.1186/s13018-024-05447-8. J Orthop Surg Res. 2025. PMID: 39773322 Free PMC article. Clinical Trial.
-
Report of the Primary Outcomes for Gait Mechanics in Men of the ACL-SPORTS Trial: Secondary Prevention With and Without Perturbation Training Does Not Restore Gait Symmetry in Men 1 or 2 Years After ACL Reconstruction.Clin Orthop Relat Res. 2017 Oct;475(10):2513-2522. doi: 10.1007/s11999-017-5279-8. Clin Orthop Relat Res. 2017. PMID: 28224442 Free PMC article. Clinical Trial.
-
Quadriceps Strength Symmetry Does Not Modify Gait Mechanics After Anterior Cruciate Ligament Reconstruction, Rehabilitation, and Return-to-Sport Training.Am J Sports Med. 2021 Feb;49(2):417-425. doi: 10.1177/0363546520980079. Epub 2020 Dec 29. Am J Sports Med. 2021. PMID: 33373534 Free PMC article.
-
The effect of knee bracing on the knee function and stability following anterior cruciate ligament reconstruction: A systematic review and meta-analysis of randomized controlled trials.Orthop Traumatol Surg Res. 2019 Oct;105(6):1107-1114. doi: 10.1016/j.otsr.2019.04.015. Epub 2019 Jul 3. Orthop Traumatol Surg Res. 2019. PMID: 31279767
-
The Effectiveness of a Functional Knee Brace on Joint-Position Sense in Anterior Cruciate Ligament-Reconstructed Individuals.J Sport Rehabil. 2016 May;25(2):190-4. doi: 10.1123/jsr.2014-0226. Epub 2015 Jan 22. J Sport Rehabil. 2016. PMID: 25611740 Review.
Cited by
-
Hybrid feature-time series neural network for predicting ACL forces in martial artists with resistive braces after reconstruction.Front Bioeng Biotechnol. 2025 May 9;13:1579472. doi: 10.3389/fbioe.2025.1579472. eCollection 2025. Front Bioeng Biotechnol. 2025. PMID: 40416312 Free PMC article.
-
Effect of knee extension constraint training on walking biomechanics 6 months after anterior cruciate ligament reconstruction: a double-blind randomized controlled clinical trial.J Orthop Surg Res. 2025 Jan 7;20(1):20. doi: 10.1186/s13018-024-05447-8. J Orthop Surg Res. 2025. PMID: 39773322 Free PMC article. Clinical Trial.
-
Functional Resistance Training Differentially Alters Gait Kinetics After Anterior Cruciate Ligament Reconstruction: A Pilot Study.Sports Health. 2023 May;15(3):372-381. doi: 10.1177/19417381221104042. Epub 2022 Jun 29. Sports Health. 2023. PMID: 35766451 Free PMC article. Clinical Trial.
References
-
- Moses B, Orchard J, Orchard J. Systematic review: Annual incidence of ACL injury and surgery in various populations. Res Sport Med. 2012;20:157–79. 10.1080/15438627.2012.680633. - PubMed
-
- Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42:2363–70. 10.1177/0363546514542796. - PubMed
-
- Van Melick N, Van Cingel REH, Brooijmans F, et al. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br J Sports Med. 2016;50:1506–15. 10.1136/bjsports-2015-095898. - PubMed
-
- Heusdens CHW, Zazulia K, Roelant E, et al. Study protocol: a single-blind, multi-center, randomized controlled trial comparing dynamic intraligamentary stabilization, internal brace ligament augmentation and reconstruction in individuals with an acute anterior cruciate ligament rupture: LIBRƎ stud. BMC Musculoskelet Disord. 2019;20:547. 10.1186/s12891-019-2926-0. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
