

Proton pencil beam scanning reduces secondary cancer risk in breast cancer patients with internal mammary chain involvement compared to photon radiotherapy
- PMID: 33008412
- PMCID: PMC7532613
- DOI: 10.1186/s13014-020-01671-8
Proton pencil beam scanning reduces secondary cancer risk in breast cancer patients with internal mammary chain involvement compared to photon radiotherapy
Abstract
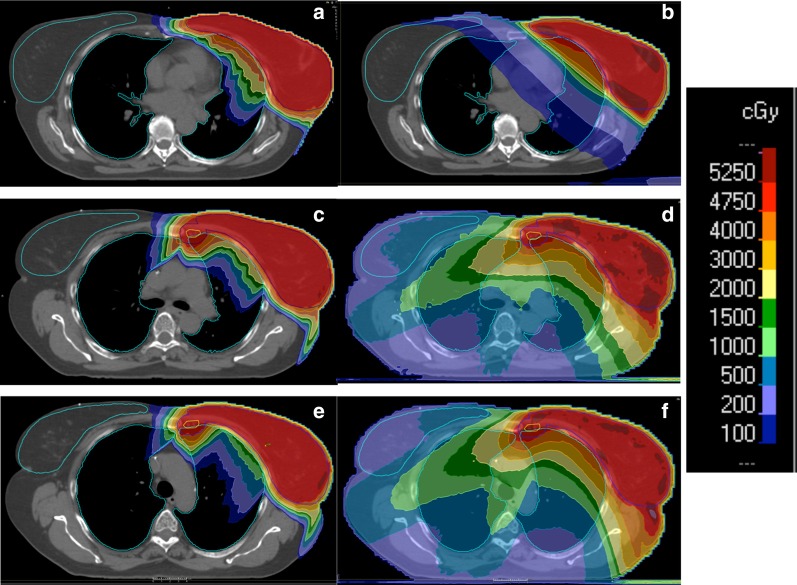
Purpose: Proton pencil beam scanning (PBS) represents an interesting option for the treatment of breast cancer (BC) patients with nodal involvement. Here we compare tangential 3D-CRT and VMAT to PBS proton therapy (PT) in terms of secondary cancer risk (SCR) for the lungs and for contralateral breast.
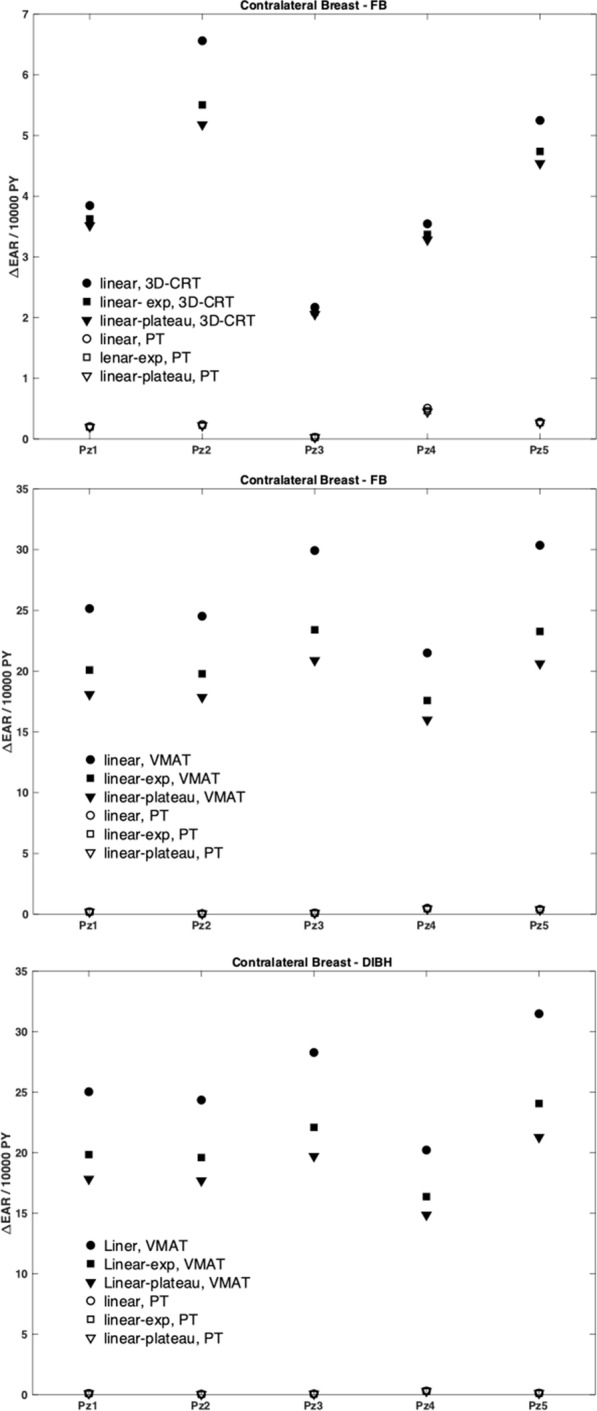
Methods: Five BC patients including supraclavicular (SVC) nodes in the target (Group 1) and five including SVC plus internal-mammary-nodes (IMNs, Group 2) were considered. The Group 1 patients were planned by PT versus tangential 3D-CRT in free-breathing (FB). The Group 2 patients were planned by PT versus VMAT considering both FB and deep-inspiration breath hold (DIBH) irradiation. The prescription dose to the target volume was 50 Gy (2 Gy/fraction). A constant RBE = 1.1 was assumed for PT. The SCR was evaluated with the excess absolute risk (EAR) formalism, considering also the age dependence. A cumulative EAR was finally computed.
Results: According to the linear, linear-exponential and linear-plateau dose response model, the cumulative EAR for Group 1 patients after PT was equal to 45 ± 10, 17 ± 3 and 15 ± 3, respectively. The corresponding relative increase for tangential 3D-CRT was equal to a factor 2.1 ± 0.5, 2.1 ± 0.4 and 2.3 ± 0.4. Group 2 patients showed a cumulative EAR after PT in FB equal to 65 ± 3, 21 ± 1 and 20 ± 1, according to the different models; the relative risk obtained with VMAT increased by a factor 3.5 ± 0.2, 5.2 ± 0.3 and 5.1 ± 0.3. Similar values emerge from DIBH plans. Contrary to photon radiotherapy, PT appears to be not sensitive to the age dependence due to the very low delivered dose.
Conclusions: PBS PT is associated to significant SCR reduction in BC patients compared to photon radiotherapy. The benefits are maximized for young patients with both SVC and IMNs involvement. When combined with the improved sparing of the heart, this might contribute to the establishment of effective patient-selection criteria for proton BC treatments.
Keywords: Breast cancer; Proton therapy; Secondary cancer risk; Tangential 3D-CRT; VMAT.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Three-dimensional conformal radiotherapy (3D-CRT) vs. volumetric modulated arc therapy (VMAT) in deep inspiration breath-hold (DIBH) technique in left-sided breast cancer patients-comparative analysis of dose distribution and estimation of projected secondary cancer risk.Strahlenther Onkol. 2023 Jan;199(1):90-101. doi: 10.1007/s00066-022-01979-2. Epub 2022 Aug 9. Strahlenther Onkol. 2023. PMID: 35943553
-
Respiratory gating for proton beam scanning versus photon 3D-CRT for breast cancer radiotherapy.Acta Oncol. 2016 May;55(5):577-83. doi: 10.3109/0284186X.2015.1120883. Epub 2016 Mar 30. Acta Oncol. 2016. PMID: 27027913
-
Left breast irradiation with tangential intensity modulated radiotherapy (t-IMRT) versus tangential volumetric modulated arc therapy (t-VMAT): trade-offs between secondary cancer induction risk and optimal target coverage.Radiat Oncol. 2019 Sep 2;14(1):156. doi: 10.1186/s13014-019-1363-4. Radiat Oncol. 2019. PMID: 31477165 Free PMC article.
-
Dose constraints in breast cancer radiotherapy. A critical review.Radiother Oncol. 2025 Jan;202:110591. doi: 10.1016/j.radonc.2024.110591. Epub 2024 Oct 19. Radiother Oncol. 2025. PMID: 39427931 Review.
-
Consensus Statement on Proton Therapy in Early-Stage and Locally Advanced Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):505-516. doi: 10.1016/j.ijrobp.2016.01.036. Epub 2016 Jan 23. Int J Radiat Oncol Biol Phys. 2016. PMID: 27084663 Free PMC article. Review.
Cited by
-
Exploring Helium Ions' Potential for Post-Mastectomy Left-Sided Breast Cancer Radiotherapy.Cancers (Basel). 2024 Jan 18;16(2):410. doi: 10.3390/cancers16020410. Cancers (Basel). 2024. PMID: 38254899 Free PMC article.
-
Internal mammary node irradiation in early breast cancer - target coverage and implications on dose to organs at risk.Acta Oncol. 2025 Jul 30;64:989-996. doi: 10.2340/1651-226X.2025.43716. Acta Oncol. 2025. PMID: 40734573 Free PMC article.
-
Heart Sparing Radiotherapy Techniques in Breast Cancer: A Focus on Deep Inspiration Breath Hold.Breast Cancer (Dove Med Press). 2022 Jul 20;14:175-186. doi: 10.2147/BCTT.S282799. eCollection 2022. Breast Cancer (Dove Med Press). 2022. PMID: 35899145 Free PMC article. Review.
-
Dynamic cardiac changes in low cardiovascular risk patients with triple negative breast cancer treated with chemo-immunotherapy.Cardiooncology. 2025 Jul 3;11(1):62. doi: 10.1186/s40959-025-00361-2. Cardiooncology. 2025. PMID: 40611344 Free PMC article.
-
Dosimetric analysis of six whole-breast irradiation techniques in supine and prone positions.Sci Rep. 2024 Jun 21;14(1):14347. doi: 10.1038/s41598-024-65461-y. Sci Rep. 2024. PMID: 38907042 Free PMC article.
References
-
- National Cancer Institute Surveillance Epidemiology and End Results Program. Cancer Stat Facts: Female Breast Cancer; 2017.
-
- Taylor C, Correa C, Duane FK, Aznar MC, Anderson SJ, Bergh J, et al. Estimating the risks of breast cancer radiotherapy: evidence from modern radiation doses to the lungs and heart and from previous randomized trials. J Clin Oncol. 2017;35:1641–1649. doi: 10.1200/JCO.2016.72.0722. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
